I fully support the idea of a National Health Service….. here is some history of how it came to be and where we are now:
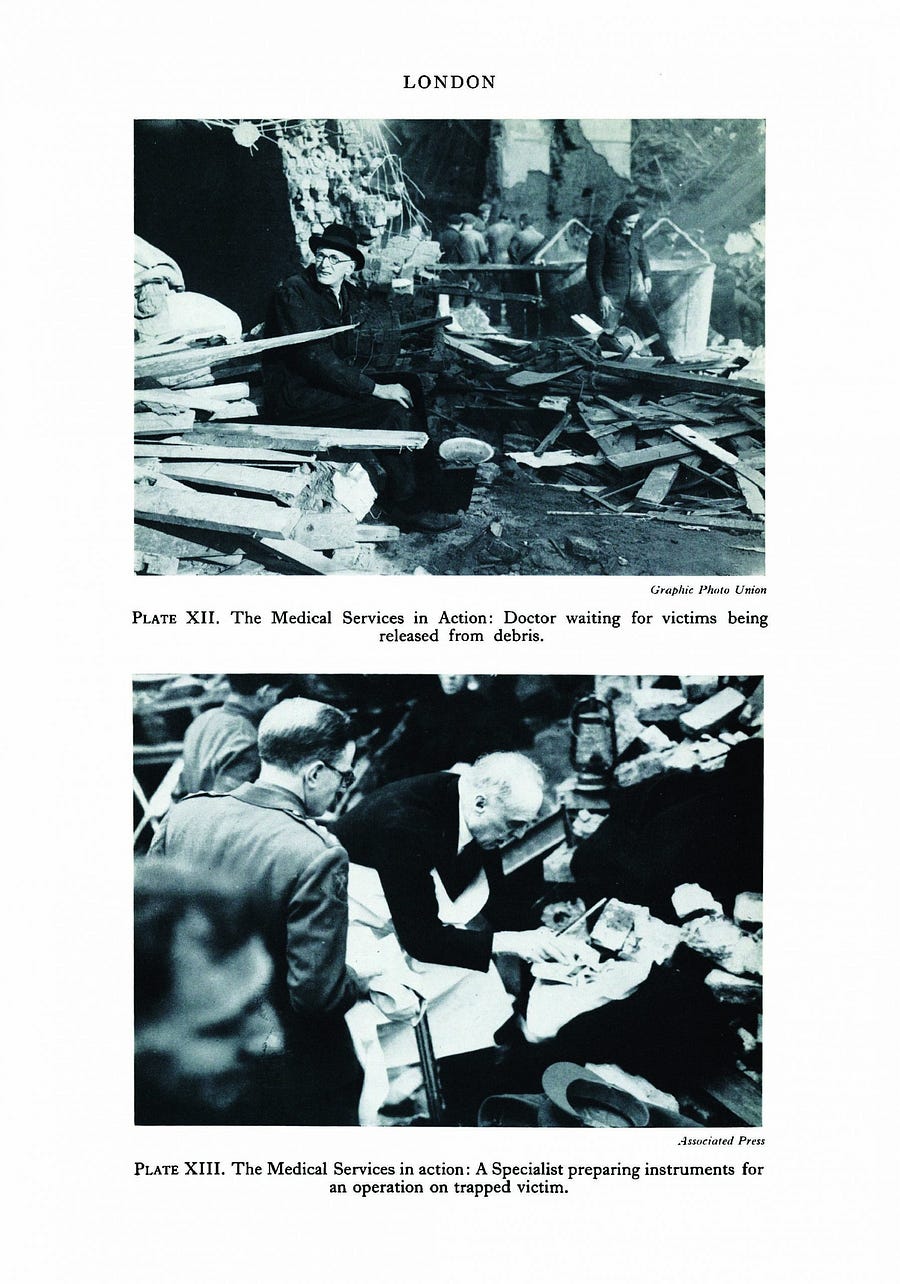
The Emergency Hospital Service (later Emergency Medical Service) was established at the outbreak of World War II in 1939, giving central government a right of direction over voluntary and municipal hospitals. The service was a loose alliance of separate organisations, working together to deal with a national emergency, but paved the way for separate and competing institutions to come together as part of the National Health Service.
The Emergency Hospital Service (later Emergency Medical Service) was established at the outbreak of World War II in 1939, giving central government a right of direction over voluntary and municipal hospitals. The service was a loose alliance of separate organisations, working together to deal with a national emergency, but paved the way for separate and competing institutions to come together as part of the National Health Service.
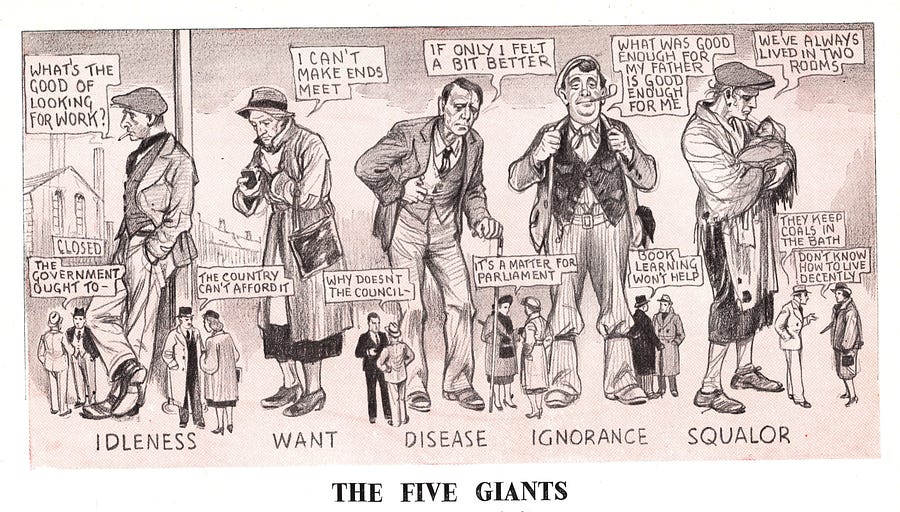
Beveridge Report (1942) recommended a government-run benefit system to help people from the ‘cradle-to-grave’. As part of the report, Beveridge set out a plan to put an end to what he called the ‘five giants’ — Poverty, Disease, Ignorance, Squalor and Idleness(unemployment). The main scheme was universal — everyone had a right to it based on contributions. There would be universal access to education and to health services. These would be funded from taxation and would be free at the point of use. Again everyone in work would pay, but in this case, since taxation increased with increasing income, the rich would pay more. The package overall gave meaning to the proud boast that the welfare state provided care for everyone — protection ‘from cradle to grave’. For it all to happen, however, there had to be full employment.
A major issue that later split the Labour Party was whether a future NHS should be run by local authorities, or quite separately on a regional basis. During the war the Conservatives produced the first White Paper on a future service in which local authorities would lead. (1944).
But after Labour’s election victory in 1945 Bevan presented to the Cabinet a radically different plan favouring nationalisation of all hospitals, voluntary or council, and a regional framework. After much tough negotiation this plan went through, with modest concessions.
The NHS Act 1946, which came into force in 1948, was welcomed by the public who were worried about the risk of epidemics spreading from other parts of the world — Measles, a highly contagious virus, for which there was no vaccine as yet, was particularly feared because in some people it resulted in blindness and brain damage.
The National Health Service started in 1948 in a society weary but disciplined by war, and accustomed to austerity.
It is difficult for us to imagine what life was like without ‘free’ health care and the difference that the
NHS made to people’s lives.
Public Health England inform NHS choices & decisions — PHE Responsibilities:
Making the public healthier and reducing differences between the health of different groups by promoting healthier lifestyles, advising government and supporting action by local government, the NHS and the public
Protecting the nation from public health hazards
preparing for and responding to public health emergencies
Improving the health of the whole population by sharing our information and expertise, and identifying and preparing for future public health challenges
Supporting local authorities and the NHS to plan and provide health and social care services such as immunisation and screening programmes, and to develop the public health system and its specialist workforce
Researching, collecting and analysing data to improve our understanding of public health challenges, and come up with answers to public health problems
NHS Constitution: The 6C’s
Another national initiative that strongly influences the Trust’s focus on providing high quality care and the Trust’s strategic direction is the 6Cs.
Nurses and midwives have signed up to deliver the 6Cs, an initiative launched by NHS England to provide compassionate and caring healthcare across all of our hospitals. The Chief Nursing Officer for England launched a three year vision and strategy for nursing, midwifery and care staff to ensure that the 6Cs are at the heart of all nursing and midwifery care.
The 6Cs are Care, Compassion, Competence, Communication, Courage and Commitment — all values essential to high quality care.
Care is our core business and that of our organisations, and the care we deliver helps the individual person and improves the health of the whole community. Caring defines us and our work. People receiving care expect it to be right for them consistently throughout every stage of their life.
Compassion is how care is given through relationships based on empathy, respect and dignity; it can also be described as intelligent kindness and is central to how people perceive their care.
Competence means all those in caring roles must have the ability to understand an individual’s health and social needs and the expertise, clinical and technical knowledge to deliver effective care and treatments based on research and evidence.
Communication is central to successful caring relationships and to effective team working. Listening is as important as what we say and do and essential for “no decision about me without me”. Communication is the key to a good workplace with benefits for staff and patients alike.
Courage enables us to do the right thing for the people we care for, to speak up when we have concerns and to have the personal strength and vision to innovate and to embrace new ways of working.
A Commitment to our patients and populations is a cornerstone of what we do. We need to build on our commitment to improve the care and experience of our patients to take action to make this vision and strategy a reality for all and meet the health and social care challenges ahead.
The Five Goals of the NHS (2015):
Preventing people from dying prematurely
Enhancing quality of life for people with long term conditions
Helping people to revoke from episodes of illness or injury
Ensuring people have a positive experience of care
Treating and caring for people in a safe environment and protecting them from avoidable harm
8 Principles, devised by RCN — on what constitutes safe and effective nursing care:
Dignity
Responsibility for own actions
Risk management
Personalised care
Communication
Up-To-Date knowledge and skills
Multi-disciplinary working
Lead by example
Groups that influence public health policy –
Government and government agencies, such as the Department of Health and Public Health have a direct influence on public health policy.
National groups, such as the government body the National Institute for Health and Care Excellence (NICE) advise doctors and the public about the most economical drugs to use. Stonewall and other “diversity groups”
Pressure groups, such as Age UK and British Heart
Foundation etc keep the needs of those they represent in the headlines, so people are more aware of what they do and how they can help.
International groups, such as the World Health Organization (WHO) and the United Nations raise awareness of global health issues. Avian flu spread across continents but because of the international awareness raised, countries were able to cope. They often overstep and try to instruct countries what to do!
I do support the NHS, but not how it has been shockingly managed since the 1980’s.
People want to blame the sitting government for all the NHS woes. But they started the moment Margaret Thatcher left office — let me explain:
The Private Finance Initiative (PFI) began life in November 1992, two years after the enforced departure of Margaret Thatcher. Chancellor Norman Lamont delivered an Autumn Statement which announced:
“…the Government have too often in the past treated proposed projects as either wholly private or wholly public. In future, the Government will actively encourage joint ventures with the private sector, where these involve a sensible transfer of risk to the private sector.”
Up to then the Tories had shown little interest in investment in public sector infrastructure, controlling “public spending in general and capital spending in particular”.
Successive Labour Chancellors had also dutifully followed the advice of the Treasury, and seen it as their role to strictly control public spending and public sector borrowing.
This resulted in mounting private sector pressure for profitable contracts to be opened up. It had also resulted in the nationalised industries being starved of funds and in-house pressure for their privatisation to escape the financial constraints.
Thatcher’s government had eagerly privatised the nationalised industries — but had prevented privatisation of the NHS, which faced an unprecedented squeeze on its budgets (since surpassed, first by the squeeze imposed from 2010).
PFI appeared to offer a way to keep public control of the services supplied in public facilities while turning to the private sector to provide funding, to take on the construction risk and to manage the facilities over the life of the asset according to a contract agreed in advance … and to generate very lucrative returns for shareholders as a result. It offered many of the benefits of privatisation to the construction and banking sector, while leaving responsibility for paying for the new buildings in the public sector, guaranteeing the flow of funds to cover the rising bills.
To embrace PFI as a policy meant breaking from rules specifically designed to guard against public sector bodies embarking upon schemes which might undermine tight controls on public spending.
However while it breached these rules, PFI was clearly in keeping with the post 1980 ideological frameworks.
Lamont’s successor as Chancellor, Kenneth Clarke, was an even more enthusiastic promoter of PFI, which he famously summed up in a 1993 speech to the CBI as:
“Privatising the process of capital investment in our key public services.”
The policy was eventually branded as the Private Finance Initiative — PFI — although the acronym was soon to be parodied as “Profits For Industry”, “Profiting From Illness,” or simply “Pure Financial Idiocy”.
PFI required projects above a certain minimum scale (in the NHS this was initially above £5m) to be opened up for bids from the private sector to finance the scheme, with repayments over a prolonged period of 25–30 years or more. Rather than owning new hospital buildings, the NHS Hospital Trusts, would become lease-holders, required to make annual, index-linked payments for the use of the building and support services provided by contractors. Hospitals built on this basis would no longer be public assets, but long-term public liabilities incurring increasing payments for a generation or more ahead. These capital schemes were not investments, but new forms of public sector debt.
NHS trust management would be left to control clinical care ONLY, while other support services including maintenance of the hospital buildings was to be done by profit-seeking private companies.
The 1990 Act had also established a new system of “capital charges” under which NHS Trusts had to pay a 6% charge on their net assets each year to the NHS Executive.
In November 1994 Clarke went further, and proposed a massive £5 billion reduction in public spending, telling the CBI conference that in future the Treasury would only provide capital for projects as a last resort — “after private finance has been explored.”
Progress on PFI contracts was slow. By July 1996 angry and frustrated CBI leaders warned Clarke that PFI could fail without more decisive action. Tory ministers believed their short Bill that was passed was sufficient — but they were soon proved wrong when one of the banks involved in the Dartford Hospital project raised doubts.
So despite all the negotiations and considerable expenditure on legal and accountancy advice, no hospital PFI schemes were signed under the government which invented PFI.
Some prominent Tories even warned that PFI might in fact prove not to be such a great idea after all.
“The government itself can always borrow money more cheaply than any private sector borrower, so the efficiency test of a private finance project has to be real………. I suspect that in the long run some of these projects will go wrong and appear again on the Government’s balance sheet, adding to public spending. We shall see.” — Norman Lamont, writing in 1999
IN COMES LABOUR:
Tony Blair won the 1997 election with a massive majority, raising high popular expectations of radical change. However, to the dismay of many, Blair’s New Labour government appointed ministers even more attentive and eager than the Tories had been to satisfy the demands of the banks.
The new government’s only legislation on the NHS in 1997 was another short Bill to facilitate PFI. The National Health Service (Private Finance) Act was pushed through with just one amendment allowed, and with one aim in mind — to “remove any element of doubt” among the bankers that, despite all the tough-sounding rhetoric insisting that PFI contracts transferred risk to the private sector — there was no real risk at all, and their money was safe.
The health minister who pushed the new Bill through parliament, Alan Milburn, made clear the Bill was intended first and foremost to give the bankers just what they wanted: “It’s about removing doubt, providing certainty, and above all getting new hospitals built”.
A Labour peer, Baroness Jay revealed who was effectively dictating the legislation: “the banks concerned have seen and agreed the wording of the Bill and have made clear that it satisfies all their concerns.”
New Labour had completely changed its position on PFI, from a sceptical rejection in 1993, to embrace the policy enthusiastically and nurture it as their own in 1997. New Labour ministers now insisted that for the “overwhelming majority of new hospitals” limited availability of public capital meant it was now “PFI or bust”.
Two years earlier Margaret Beckett, as shadow health secretary, had toughened up Labour’s critical response, telling the Health Service Journal: “As far as I am concerned PFI is totally unacceptable. It is the thin end of the wedge of privatisation.”
But in the summer of 1996 Shadow Treasury minister Mike O’Brien announced a reversal of New Labour’s policy: “This idea must not be allowed to fail. Labour has a clear programme to rescue PFI”
The “rescue of PFI” was duly included in New Labour’s 1997 manifesto, sitting strangely alongside promises to scrap the NHS internal market. The pledge to scrap the market rather predictably proved to be an empty one: but the promises to implement PFI were sincere enough. By the spring of 1998, PFI was declared to be: “A key part of the [New Labour] Government’s 10 year modernisation programme for the health service.”
While Kenneth Clarke had openly boasted that PFI would generate new profits for the private sector, New Labour, insisted using private investment to modernise public services was a “partnership,” an example of the ‘Third Way’ , finding common ground between neoliberalism and social democracy. Despite its popularity with New Labour ministers (most notably with the Treasury team) PFI soon began to incur the increasingly vociferous opposition of the BMA, the Royal College of Nursing, UNISON and almost all trade unions, local campaigners in affected towns and cities, and a growing body of academics.
PFI came to be associated with funnelling profits to the private sector and contracting out/privatisation of support services. Nevertheless as soon as the 1997 Act went through Parliament the go-ahead was suddenly given to 15 hospital projects in 1997, prior to devolution, so the first list of schemes agreed included one in Wales and three in Scotland.
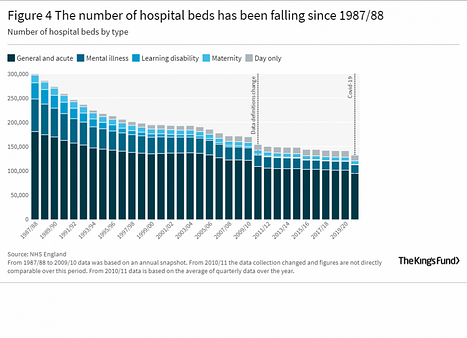
17 of the first 22 PFI hospitals were costed at below £100m. Even including the more expensive schemes the first wave schemes averaged less than £100m each. However most first wave PFI hospitals — which in most cases brought sharp reductions (ranging from 20%-40%) in bed numbers — struggled both financially and clinically as a result of flawed schemes. Several of these same schemes are still in severe difficulties now, 23 years after the first of the PFI hospitals opened.
The bed reductions came from a combination of efforts to hold down costs by restricting the scale of the new buildings on the one hand, and on the other hand the involvement of management consultants committed to the introduction of “innovative methods,” who made hugely over-optimistic assumptions on the increase in throughput of patients per bed that could be achieved through the move to a new building — and sharp reduction of average length of stay.
In Worcestershire, for example, the PFI scheme, shaped by management consultants SECTA and the propositions put forward by the King’s Fund, sought to reduce bed numbers by 35%, and cut beds per 1,000 patients by 40%. This meant hoping for a truly massive increase in throughput per bed by reducing average length of stay — without any actual evidence that this could be achieved.
“While Kidderminster faces the loss of 100% of its acute in-patient beds, the whole of Worcestershire also faces a massive, possibly unprecedented cutback in acute beds under the WHA plan. Figures in the supporting documents show that the combination of the Kidderminster rationalisation, the Worcester PFI scheme and the WHA “efficiency” measures would close up to 35% of the county’s front-line acute beds in just four years. There are no grounds to assume that hospital services would be able to cope with such a massive and rapid cutback.” John Lister of London Health Emergency
To make matters worse it was difficult to get any detailed or serious public discussion or political critique of specific issues and schemes: the media remained largely oblivious to the whole question of PFI, and MPs and pro-PFI enthusiasts were keen to brush aside and ridicule any critics of the scheme, dismissing them as negative opponents of building a new hospital.
In one South East London trust, Queen Elizabeth Hospital, Woolwich, which opened in 2002, the scale of the financial problem reached the level of ‘technical bankruptcy’ just 3 years later, with the trust paying out 14.5% of its income on the “unitary charge” for use of the building and support services, according to a 2005 Audit Commission report. John Lister for UNISON
PFI also failed to deliver on another measure of value for money: many staff working in the new hospitals, especially the first wave PFI hospitals, were profoundly unimpressed by the quality and design of the buildings, criticising predictable practical problems, compounded by the limited or non-existent prior engagement with staff in drawing up the plans, and the failure to learn lessons from the first hospitals before completing plans for others with similar problems.
ALL of the first-wave PFI hospitals are desperately short of beds, with an immediate consequence for nursing staff who are under pressure to discharge patients more quickly. Several of these hospitals — all opened since 2000 — are already looking to build new extensions, or are resorting to the use of Portakabins, old buildings that should have been demolished, or local private sector beds to bridge the gap in capacity that has opened up.
So in my Happy Birthday wishes to the NHS, I also hope for someone — anyone in power to roll back the harmful Labour PFI initiatives, and every other harmful piece of Labour, Lib Dem and Tory legislation and Policy since — that further sinks the NHS into the abyss of debt to private organisations!
2000 New Labour’s NHS Plan introduces private provision of medical services into the NHS for the first time to ‘modernise’ and ‘reform’ its practices. Routine planned surgery, diagnostic tests and procedures are contracted out to private sector treatment centres at greater cost than the same care on the NHS.
2003 New Labour allows NHS trusts to apply to become Foundation Trusts (FTs), arms-length business entities independent of government control. This further embeds commercial priorities and leadership into the system.
2004 New Labour brings in Payment by Results. Providers are paid a fixed price per unit of completed health care. This helps the private sector to cherry-pick the easiest, most profitable treatments.
2009 Gordon Brown (New Labour) brings in the Unsustainable Provider Regime, the framework for using the PFI hospital debt burden to close and sell off publicly-owned NHS land and property.
2012 David Cameron & Nick Clegg’s (Conservative / LibDem coalition) Health and Social Care Act (HSCA) abolishes the legal foundation of the NHS, removes the Secretary of State for Health’s legal duty to provide healthcare for all, hands responsibility to a series of new quangos — most notably NHS England (NHSE) — and opens all major NHS contracts to the private sector. This accelerates private involvement in the NHS and substantially increases administration costs.
2013 The Conservative / LibDem coalition replaces Primary Care Trusts (PCTs) with new, GP-run Clinical Commissioning Groups (CCGs), transitional state-owned-and-run insurance pools based on American private Health Maintenance Organisations. 60% of NHS budgets flow through CCGs.
2014 The Conservative / LibDem coalition appoints Simon Stevens, former head of the global division of American health insurance giant UnitedHealth, as Chief Executive of NHS England to manage the final stage of privatisation; the coalition continue to support his efforts. Stevens spends £millions embedding UnitedHealth’s UK subsidiary Optum and US ‘managed care’ in England. He oversees the introduction of Optum software, algorithms, personnel, business practices, and the training of local council leaders to replicate American Medicare, which will reduce England’s NHS to a funding stream and a logo.
Stevens publishes his Five Year Forward View (FYFV) introducing Sustainability and Transformation Plans (STPs) and New Models of Care, creating the impression that these are NHS sanctioned policy. The narrative of ‘integration’ points to a move to Accountable Care Organisations (ACOs), based on the American private insurance industry-devised model. The plan is to:
Reduce the number of full A&E hospitals from 140 (in 2013) to between 70 and 40
Reduce the number of GP surgeries from 7500 to 1500 “superhubs”
Close smaller hospitals to produce economies of scale and cut future private sector costs
Shrink provision of expensive, high risk, unprofitable healthcare to the sickest patients
Consolidate lower risk routine planned healthcare ahead of outsourcing
2015–17 Stevens rolls out STPs, dividing NHS England into 44 regions or Footprints to be run by ACOs (now re-named Integrated Care Systems — ICSs).
2016 Junior doctors strike over a new contract adversely affecting pay, part-time female doctors, and more anti-social working hours that put lives in danger. Exercise Alice, a dry-run of how the NHS would respond to a coronavirus-like pandemic, identifies the need for more trained NHS personnel, beds and Personal Protective Equipment (PPE) as well as the need to maintain contact tracing and patient isolation capacity. Both Theresa May’s government (Conservative) and Simon Stevens fail to implement these recommendations.
2017 The Naylor Review report by global accounting consultant Deloitte & Sir Robert Naylor for the Conservative Secretary of State for Health, and Project Phoenix, create incentives for Trusts to sell NHS land and assets as the only option to raise funds to buy, improve and maintain hospitals, equipment and NHS properties.
2018 The Commissioning Capabilities Programme run by UnitedHealth / Optum in partnership with global accounting consultant Price Waterhouse Cooper (PwC), is an exercise setting out the curriculum and all the design functions for both advanced and aspiring ICSs.
2019 A major new contract for GPs means they are grouped together to form Primary Care Networks (PCNs), which form the foundation of American-style Integrated Care. Managers and computer software (rather than doctors) determine ‘care pathways’ for patients and decide on treatments. The British Medical Association (BMA), the doctors’ union, wave through the contract binding GPs in to PCNs, with hardly any debate and no vote of GPs.
2020 Under Boris Johnson (Conservative), NHS privatisation, the decision by Theresa May’s government and Simon Stevens not to prepare for pandemics, and Covid19 create a perfect storm. Hospitals become emergency Covid treatment centres. GPs are instructed by NHS England (NHSE) to replace face-to-face appointments with phone consultations, making it almost impossible to see a GP — a taste of what’s to come under American-style ‘managed care’. More than 1,500 health and care staff die from Covid due to the lack of PPE, the unofficial Tory ‘herd immunity’ policy, delayed lockdowns etc. The Conservatives pay two corporations without any expertise in public health — global accounting consultant Deloitte and outsourcing giant Serco — £37 billion to set up Test & Trace, which makes ‘no measurable difference’. Sir David King, former government Chief Scientific Officer, estimates that more than 100,000 UK Covid deaths could have been avoided.
2021 The Conservative’s Health and Care Bill revises the number of ICSs to 42. Each ICS board will serve private corporate interests, control all spending and decide what treatments to allow patients in their region. As with US ‘managed care’, the more private corporations cut and deny care, the more profit they’ll make. The Bill removes Section 75 of HSCA to allow private companies to be awarded £multi-billion contracts behind closed doors without competition, normalising what went on during the pandemic with PPE and Test & Trace.
2022 The Health and Care Act puts ICSs on a legal footing. From July 1st, ICSs start operating throughout England, effectively de-nationalising the English NHS. Waiting lists top 7 million, the highest since records began. NHS wage stagnation, the cost of living crisis and rampant inflation lead hospital trusts to open food banks for nurses and junior doctors who are going hungry. This, together with a new round of austerity imposed by Rishi Sunak‘s government (Conservative), leads NHS nurses to vote to strike against low pay and patient safety concerns for the first time in their history. They are soon joined by ambulance drivers and paramedics for similar reasons.
2023 Junior doctors strike for full pay restoration (after losing around 30% of their income since the Conservatives took power in 2020), safeguards against inflation and reforms to protect the recruitment and retention of junior doctors.
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behaviour or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.