Apotemnophilia, Paraphilia or Body Integrity Identity Disorder (BIID), Dysphoria Resolved by Self-Amputation (GB 1992): Case-History 12-Year Follow-Up (2009) with Medical Ethical Issues— to 2023
Body integrity dysphoria (BID, also referred to as body integrity identity disorder, amputee identity disorder and xenomelia, formerly called apotemnophilia)
G. F. Pranzarone, PhD Professor of Psychology, Sexologist Roanoke College Psychology Salem, Virginia FSWVAAP, April 25, 2009 — Adapted and added to by Mia @_CryMiaRiver Ottawa, Ontario & Jen @JenKTeach England, UK
Shooting Off A Leg
George carried a shotgun to the woods behind his apartment — ”To shoot crows” was the cover story.
He was giddy with the prospect of obtaining the long desired amputation of his left leg.
He had learned by shooting hams and legs of lamb, where to place the muzzle just above the knee so the blast would do the most damage.
He felt impact rather than pain. Pain would occur in the EMS vehicle on the way to the hospital.
After 14 days of argument, his leg is amputated.
He experiences joy for 12 years until his death at 79.
George’s Characteristics
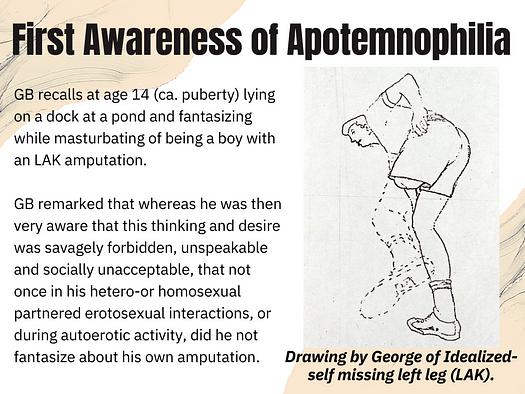
George (GB) first seen as a 64-year-old bisexual male with multiplexed paraphilias of ephebophilia, rubber fetishism, and apotemnophilia experienced in his sexuoerotic ideation and fantasy since age 14 years.
Twice married and divorced, with wives and children estranged due to their inability to accept — and from embarrassment over — his public expression (as in “National Enquirer”) of a desire for self-amputation.
GB was brilliant, articulate and cultured, a university graduate, who studied prosthetics and worked as an architect and entrepreneurial businessman. Not psychotic or delusional.
Pathology of Mother-Child Interaction
At age 3 years a pot of boiling oatmeal was upended onto GB’s left shin and foot producing severe burns. His scarring and recovery involved his limping and overly solicitous care by the mother.
GB was emotionally outraged at what he described as a mother-child relationship in which the mother was overly intrusive and emotionally incestuous. “There was no boundary between her and me. She would say we have no secrets do we George?”
His outrage endured a lifetime as expressed during psychotherapy in the latter part of his life. The topic of his mother caused him to become emotional to the point of trembling. “She would not let me become myself!”
Love-map Imprinting Events
GB’s older brother was athletic and a father’s favourite whereas he was not and was chided by his father for his ineptness in sport. At age 8 he was taken by his father to a baseball game at which he witnessed for the first time, with terror and excited fascination, a 12 year-old boy with a peg-leg and crutch, stand at home plate, hit a ball, and exuberantly run the bases. GB’s amazement and admiration converted into identification in which he desired to become the boy who successfully overcame his handicap.
His father asked an older boy to befriend young GB. He would take GB into the woods to walk a trap-line. GB remarked that he witnessed several cases of animal limbs left behind when the trapped animal gnawed off the leg to allow it to escape.
George often spoke and wrote of poet William Blake’s dictum: “You become what you behold.”
He and the older boy became very close . When the friend left town GB entered a profound depression. At 12 years of age a local pastor consoled and revealed to GB that his affection and love for his departed friend was probably due to a non-sexual gay relationship (homophilia).
GB became increasingly aware of his bisexuality over years of psychotherapy. GB consequently self-identified as a gay ephebophilie — most attracted to later teen or younger men. The love of his life was a young physician who died after years of a mutually rewarding relationship.
Dysphoria of Apotemnophilia
GB went on to college, graduated, and entered the army. He was later discharged due to homosexual activity. Even then he did not speak of the desire for amputation to the counsellors. He felt that an unspeakable monster existed within.
During his marriages and careers the one consistent element in life was his fascination and obsession with his becoming an amputee. This fixation (idee fixe) was so overwhelming and demanding a desire that GB sought therapy for resolution and relief from this compulsive “need.” GB differentiated between a simple desire and this tormenting “need.”
Apotemnophilia Refractory to Therapies
GB kept meticulous diaries re: his condition and his corresponding cognitive and affective states. He sought to understand the etiology, progress and possible resolution of his own syndrome. GB spent considerable effort and funds in attempts to resolve his demanding and personally unacceptable desire for amputation.
He submitted to various forms of psychodynamic therapies, behavioural aversion training and a two-year period of self-admission to Austen Riggs Center in Stockton, MA. Albert Ellis’ REBT, did not change GB’s desire for self-amputation, but did allow successful self-acceptance. GB realized he was not living in an awful, unbearable situation and was not a terrible person deserving of condemnation for being an apotemnophile. While at the REBT Institute in NYC, he dated a woman amputee who found GB an acceptable companion.
OCD medications did not provide relief from his fixation. Depo-Provera ameliorated the strength of the sexuoerotic link of amputation fantasy to arousal and achievement of orgasm, but GB found the lowered libido unacceptable. GB remarked that some therapists distanced themselves from his case or would not treat his apotemnophilia either from ignorance of the syndrome or from fear of litigation should he succeed in self-amputation during the therapy.
Dysphoria and Decision to Self-Amputate
At age 67 GB’s fixation and dysphoria was overwhelming. He studied anatomy and with Lidocaine drove sharpened metal rods smeared with faeces and nasal mucus through the front of his left knee into the medulla of his tibia. This was an attempt to produce osteomyelitis, which he knew often required an amputation.
After a course of infection and pain that was near unbearable, GB appeared at a hospital ER expecting the sought-after amputation. However, the infection was resolved by drainage and antibiotics.
GB became suicidal. Driving on the highways in his sales work he pounded his left leg just above the knee with rocks to produce hematomas.
He contacted other apotemnophilies and read newsletters (e.g., “ParaAmps”) and learned of Dr John Money’s Psychohormonal Research Laboratory at Johns Hopkins Medical School in Baltimore. A call began three years of visits to Dr Money.
GB learned that apotemnophilia was a paraphilia, a distortion of normal love-map development by its vandalization in pathologic childhood events and interactions. George was blameless in his apotemnophilia, a medical syndrome, one of 50+ paraphilias.
GB remarked that in the depth of his depression “John Money saved my life. . . with his compassion, non-judgmental acceptance, understanding and advice.”
“Hunting Accident” & Surgical LAK Amputation
At age 67 GB was determined to achieve an amputation. He would die rather than continue to live with an unacceptable body image.
He practiced on legs of lamb and ham with a shotgun to learn the optimum muzzle distance from the leg to produce the most damage.
One day a week short of Thanksgiving 1993, he entered the woods behind his apartment “To shoot crows” with an owl decoy (which crows attack), a portable phone to call 911, materials for a tourniquet, and the shotgun. He seated himself on a log with the gun aimed above his left knee and pulled the trigger.
The discharge was felt as an impact. He remembers that the shot made a mess of blood, fat, tissue and bone splinters. He placed the tourniquet and dialled 911 but had walked beyond the phone’s range. Fortunately, his landlady heard the shot, came to investigate and called 911. Pain did not occur until later within the EMS vehicle.
In hospital GB awakened to find to his dismay that the leg remained attached but bandaged.
Desired Surgical LAK Amputation Achieved
The orthopaedist suggested that the leg could be fused intact. It would heal shorter, carry his weight, but would not bend at the knee.
GB argued that the shorter-stiff leg would be more inconvenient than an amputation with a prosthesis. A psychiatrist was asked to evaluate him but GB knew what to say so as to present a non-psychotic persona.
George prevailed, and the leg was amputated on the 14th day post-trauma.
Post-Amputation Sequalae
After healing, a prosthesis was fitted and George realized a secondary benefit to his amputation — the latex rubber socket that fit over his stump had an erotic component.
The sexuoerotic potential of his LAK stump also became apparent and actualized. Rubbing the stump could be felt as sensations in his penis. An orgasm could be felt in his stump.
This erotic component of stumps has been reported by neurologist V.J. Ramachandran in other amputees, who usually did not seek their amputations but were amputated after accidental trauma or disease.
Counselling about issues surrounding his mother, who lived to be 100+, and depression over other health issues (COPD) was obtained for the remaining years of his life. George’s therapist reported that the amputation 12 years earlier was life transforming as if in a healing of a long endured debilitating illness. A calming occurred and the agitation and dysphoria George endured over possession of his intact leg had ended.
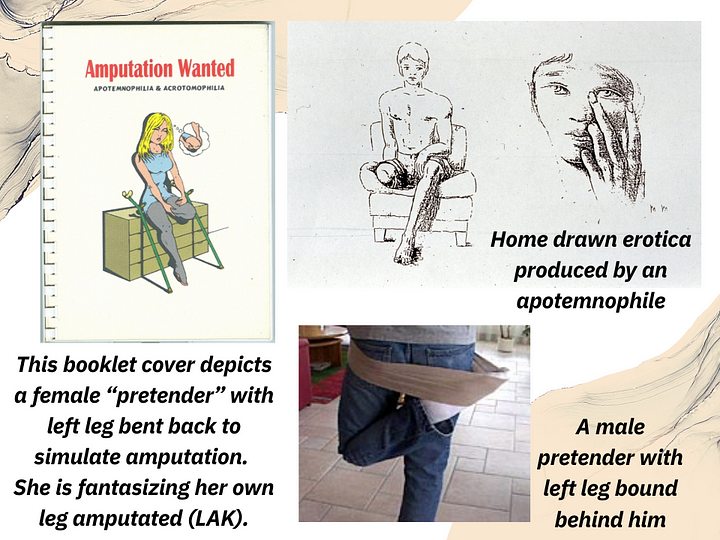
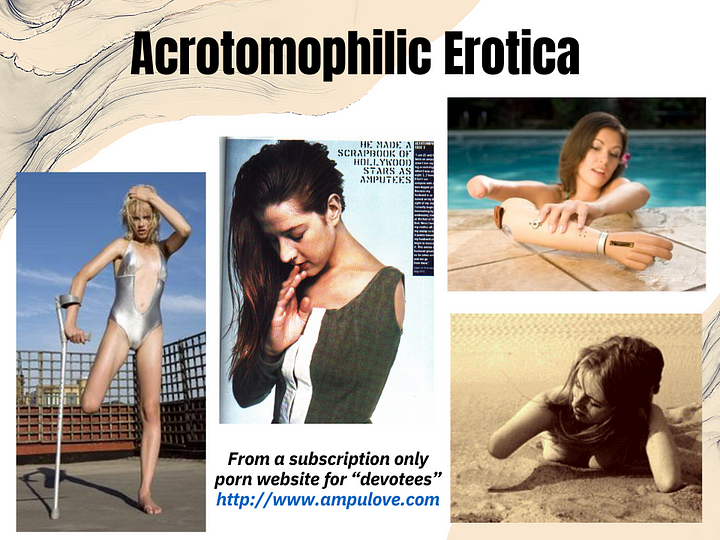
With a computer GB began years of serving as a guru and advisor to online “Devotees, Pretenders, and Wannabes“ on the many websites for apotemnophilies and acrotomophilies. In his last years GB became affiliated with a Jewish community and after study was officially converted at his Bar Mitzvah. George Boyer died in September 2004, of pneumonia after a hip fracture. He had a history of COPD.
Sequalae: Pride in the Amputation
George was theatrical about his LAK amputation. He favoured shorts in public to display his stump and prosthesis. He delighted in the glances of passers-by and happily explained his stump & “C-leg” articulation to children who seemed not so put-off as were the adults. This theatricality is also seen among transgendered persons who actualize transition to their concordant sex through SRS.
George was profiled in articles & videos for television & theatre, TLC’s Legs, a BBC documentary called A Love Apart, & Whole by Canadian Melody Gilbert. Asked about whether he had regrets in his life, George responded, “My only regret is that I suffered 67 years and did not act sooner to get rid of the leg. I have loved my life since then. I am now who I always wanted to be — myself.”
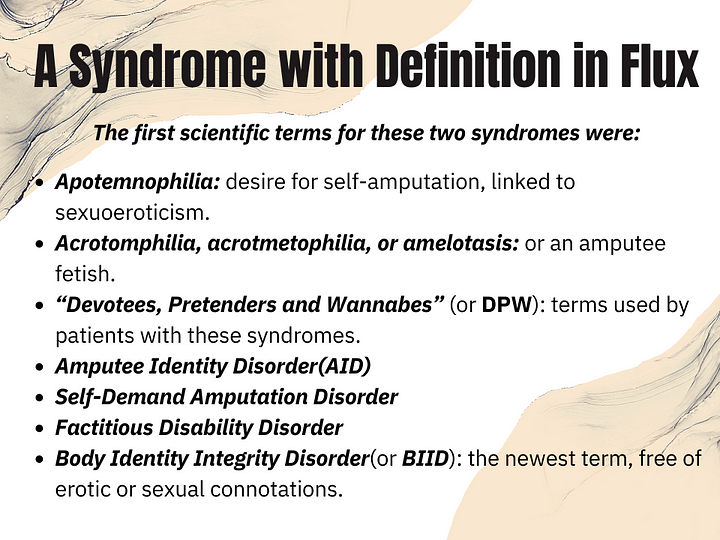
Apotemnophilia vs. BIID (2010)
Apotemnophilia better applies in the case of George rather than the asexual “Body Integrity Identity Disorder” (BIID) for the DSM-V (2010).
BIID is similar to transgenderism in that the gender identity/role of an individual is incongruent with his or her morphological sex.
In both syndromes the sexuoerotic component is minimized and dysphoria relates to not possessing the desired body morphology.
Removal of the sexuoerotic component in BIID, in the proposed DSM-V (2010) definition, makes the syndrome socially acceptable, as is transgenderism when compared to homosexuality.
The syndrome no longer identified as a paraphilia, thus facilitates medical intervention as is done in transgendered persons who undergo protocols for psychological evaluation, real-life tests, hormone therapy and sexual reassignment surgery (SRS).
BIID or apotemnophilia is NOT a variant of Munchausen’s Syndrome.
Apotemnophilia vs. BIID (2023)
Body integrity dysphoria (BID, also referred to as body integrity identity disorder, amputee identity disorder and xenomelia, formerly called apotemnophilia) is a mental disorder characterized by a desire to have a sensory or physical disability or having discomfort with being able-bodied beginning in early adolescence and resulting in harmful consequences.
BID appears to be related to somatoparaphrenia (a type of delusion where one denies ownership of a limb or an entire side of one’s body. Even if provided with undeniable proof that the limb belongs to and is attached to their own body, the patient produces elaborate confabulations about whose limb it really is or how the limb ended up on their body). People with this condition may refer to themselves as “trans-abled”.
Apotemnophilia vs. BIID (1980–2023)
Prior to the release of the ICD-11, the diagnosis of BID as a mental disorder was controversial. There was debate about including it in the DSM-5, and it was not included; it was also not included in the ICD-10.It has been included in the ICD-11, which reached a stable version in June 2018, as ‘Body integrity dysphoria’ with code 6C21
There is still debate and a non-consensus to the latest DSM IV classifications
DSM-III through DSM-IV — The term paraphilia was introduced in the DSM-III (1980) as a subset of the new category of “psychosexual disorders.”
The DSM-III-R (1987) renamed the broad category to sexual disorders, renamed atypical paraphilia to paraphilia NOS (not otherwise specified), renamed transvestism as transvestic fetishism, added frotteurism, and moved zoophilia to the NOS category.
It also provided seven non-exhaustive examples of NOS paraphilias, which besides zoophilia included exhibitionism, necrophilia, partialism, coprophilia, klismaphilia, and urophilia.
The DSM-IV (1994) retained the sexual disorders classification for paraphilias, but added an even broader category, “sexual and gender identity disorders,” which includes them. The DSM-IV retained the same types of paraphilias listed in DSM-III-R, including the NOS examples, but introduced some changes to the definitions of some specific types.
The DSM-IV-TR describes paraphilias as “recurrent, intense sexually arousing fantasies, sexual urges or behaviours generally involving nonhuman objects, the suffering or humiliation of oneself or one’s partner, or children or other nonconsenting persons that occur over a period of six months” (criterion A), which “cause clinically significant distress or impairment in social, occupational, or other important areas of functioning”
(criterion B). DSM-IV-TR names eight specific paraphilic disorders (exhibitionism, fetishism, frotteurism, paedophilia, sexual masochism, sexual sadism, voyeurism, and transvestic fetishism, plus a residual category, paraphilia — not otherwise specified).
In the current version of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR), a paraphilia is not diagnosable as a psychiatric disorder unless it causes distress to the individual or harm to others.
Bioethics professor Alice Dreger interpreted these changes as “a subtle way of saying sexual kinks are basically okay — so okay, the sub-work group doesn’t actually bother to define paraphilia. But a paraphilic disorder is defined: that’s when an atypical sexual interest causes distress or impairment to the individual or harm to others.”
Interviewed by Dreger, Ray Blanchard, the Chair of the Paraphilias Sub-Work Group, stated, “We tried to go as far as we could in de-pathologizing mild and harmless paraphilias, while recognizing that severe paraphilias that distress or impair people or cause them to do harm to others are validly regarded as disorders.”
Ethical Issues for Physicians — Hippocrates: “First, do no harm.”
Dr. Christopher Ryan, MD, psychiatrist at University of Sydney, argues for allowing patients with apotemnophilia (BIID) to have elective amputations. According to Dr. Ryan, doctors have a moral duty to amputate for the health and safety of the patient.
Dr. Ryan said such operations are like plastic surgery. Elective amputation would be offered to BIID sufferers only. “Unless these patients know that doctors will take their concerns seriously, and at least consider their requests, more people will risk their lives trying to remove their own limbs.” One 30-year-old patient lived his life feeling he was truly an amputee, but was so ashamed of how he felt he did not tell anyone. “Eventually he took the only step he thought he had open to him and placed his leg in a bucket of dry ice until it died and had to be removed,” Dr Ryan said. “Now, a year later, he is living happily as an amputee and getting on with his life.”
Dr. Robert Smith, MD, a surgeon in Scotland has amputated healthy legs from two patients with BIID and had six BIID candidates waiting. Scottish politicians called the procedure “obscene” and discovered that one of the men Smith operated on ran an amputee fetish website. Upon investigation, the hospital deemed the procedures unethical; Smith was banned from mutilating healthy bodies, and the ethically dubious experiment ended.
Ethical Medical Practice – For Amputation?
Discussions of violations of ethical practice are now occurring regarding amputation of healthy limbs to otherwise reduce psychological dysphoria and stress. How does this differ from healthy women who elect double mastectomies from fear of the likelihood (not certainty) of cancer? How does this differ from plastic surgery (rhinoplasty, labioplasty, breast-enhancement/reduction, SRS, or liposuction, to enhance self-regard in cases of poor body-image?
Would it be malpractice for a surgeon to amputate a BIID patient ? — GB’s delayed but otherwise successful resolution of his BIID-Apotemnophilia dysphoria by amputation, support a proposition that direct surgical intervention to actualize a patient’s desired body morphology be considered as a beneficial and ethical medical procedure. A protocol such as the Harry Benjamin Standards for Gender Identity Disorders should be established for apotemnophilies or BIID sufferers.
Ethical Medical Practice — For Treatment?
Although BIID is not considered a psychotic disorder, it may oftentimes be treated with a standard medication for a psychotic disorder. Second generation antipsychotics have been known to help with symptoms of OCD and major depressive disorder. Rhere has been at least one person that was suffering from BIID and had taken Risperidal who showed significant improvements in the desires for amputation. In turn, this patient reported having far less desire to be an amputee after being on this medication. Trying one or more medications from this classification could be beneficial.
Secondary symptoms of BIID can range from depression to OCD. Dr. First and his sample reported that if there was a secondary symptom to the BIID, it should be treated as such. If a patient suffers from depression, that particular mental disorder should be treated first and foremost on its own. Antidepressants and sometimes other antipsychotics are used alone or in conjunction with one another to correct the problem. Once a plan of attack is sorted out and everything is figured out, the quality of life of someone suffering from BIID may become better due to mood changes.
Virtue ethics conformity of one’s life and conduct to moral and ethical principles; uprightness; positive behaviour (Your morals, the importance of role models )
One of the first theories of ethics stems from the work of Plato and Aristotle, and focuses on the moral character, or virtues, of the individuals. This theory of ‘Virtue Ethics’ would apply in a health or social care setting based on the professional, who would make decisions based on their morals. What they feel is the right way to behave towards patients and colleagues. Virtue ethics relate to the internalised moral characteristics, rational thought and practical wisdom of a virtuous person who possesses and lives the virtues. The traits must be possessed as stable, fixed and reliable. While this is a particularly attractive value in healthcare professionals there is debate over how, when and to what extent these virtues are acquired and how they are influenced by societal values. For example, you might take time to explain treatment options to a patient, asking them how they feel about possible treatment options or what is going to happen, and involve them in decision-making processes. The challenge with this form of ethics can be the lack of clear guidance. The requirement to act “as a virtuous person would act given the situation” can make it difficult to identify the morally correct course of action where more than one alternative may be open to the practitioner and patient. National Advisory Group on the Safety of Patients in England (Aug 2013).
Consequentialism the theory that ethical decisions should be made on the basis of the expected outcome or consequences of the action. Ethical actions were ones that caused the most possible happiness and the least possible pain (Greater benefit to greater number of people)
Another ethical theory and approach is Consequentialism. Early writers on consequentialism were Jeremy Bentham (1748–1832) and one of his students, John Stuart Mill (1806–1873). A modern writer on consequentialism is Peter Singer (born 1946). This theory says that the correct moral response is related to the outcome, or consequences, of the act, not its intentions or motives. If you were making a decision about a person’s health or social care using this theory, you would look at the likely results of your decision for that person’s wellbeing and the wellbeing of others. For example, a critically-ill child needs a very expensive surgical treatment and has low survival expectancy. Should the NHS do the operation or should the money be allocated to carry out hundreds of tonsillectomy operations? What are the consequences of spending the money either way? Which is the most important? (Billingham et al., 2016) One famous way of putting this is ‘the greatest good for the greatest number of people’. The most common forms of consequentialism are the various versions of utilitarianism, which favour actions that produce the greatest amount of happiness. Despite its obvious common-sense appeal, consequentialism turns out to be a complicated theory, and doesn’t provide a complete solution to all ethical problems. Two of the main issues with consequentialism are; that it can lead to the conclusion that some quite dreadful acts are good, what one person feels is in the best interests of many, may result in the loss of life for others. Also that predicting and evaluating the consequences of actions is often very difficult and though we may think we are acting for the benefit and the greater good of many, we may in fact be causing more harm in the long run.
Deontology ethics, especially that branch dealing with duty, moral obligation, and right action. It focuses on your intentions rather than the outcomes of your actions. (Intentions, laws and legislations)
Deontology is often seen as being strongly opposed to consequentialism. This is because in emphasising the intention to act in accordance with our duties, deontology believes the consequences of our actions have no ethical relevance at all. As an ethical approach Deontological ethics are based on duties and rights and respect individuals as ends in themselves. It places value on the intentions of the individual (rather than the outcomes of any action) and focuses on rules, obligations and duties. Deontology requires absolute adherence to these obligations and acting from duty is viewed as acting ethically. NHS Education for Scotland. (01-May-2018) One of the key criticisms in healthcare is that applying a strictly deontological approach to healthcare can lead to conflicts of interest between equally entitled individuals which can be difficult or even seemingly impossible to resolve.
Principlism A system of ethics based on the four moral principles of autonomy, beneficence, non-maleficence, and justice. Linked to idealism. (Person centred approach)
Writers on principlism include Tom L. Beauchamp and James F. Childress. This approach uses the following four key ethical practices;
Autonomy: respecting the decision-making capabilities of autonomous people by enabling them to make independent, reasoned and informed choices about their own care.
Beneficence: balancing benefits of treatment against the risks and costs, so acting in a way that benefits the patient and promotes the wellbeing of others. For example, using the cancer drug trastuzumab (Herceptin®) costs £22,000 to treat one person for one year (correct in August 2015). Would this money be better spent on saving many people who suffer a heart attack each year?
Non-maleficence: doing no harm, so avoiding causing harm. For example, by making sure that any side effects of a treatment do not outweigh the benefits of that treatment.
Lastly, Justice: being morally right and fair, distributing a fair share of benefits, doing what the law says and looking at the rights of the people involved. (Billingham et al., 2016).
The aim of principlism is to bring together the best elements of the various other ethical theories that match with most social, individual or religious belief systems. This theory is most commonly and widely used within the Health and Social Care sector. In recent years, respect for patient autonomy has assumed great significance in the context of patient choice, underpinned by the requirement to provide the patient with sufficient information to put him/her in a position to choose. The ‘Four Principles’ are intended as an aid to balance judgement, not a substitute for it. UK Clinical Ethics Network (2019)
In conclusion, these theories give professionals a structure or framework to guide them, alongside professional codes of conduct when making difficult ethical decisions. We may feel instinctively that a certain conclusion to a problem is ‘fair’ or ‘unfair’, but without set criteria, how do we use this to make such judgments?
These different ethical theories can be applied to a problem to enable our thinking process to follow and form a clear plan of action, even if the results may not fit with our moral intuition. Our morals after all may vary between those of other professionals, so these theories help us to reduce conflicts within a professional setting.
Where next?
As of 2014 the cause was not clear and was a subject of ongoing research. However a small sample of people with body integrity dysphoria connected to their left leg have had MRI scans that showed less grey matter in the right side of their superior parietal lobule. The amount of grey matter missing was correlated to the strength of the patients’ desire to remove their leg.
If we apply the current research linked to ADHD and neurological issues for many people who present with BIID, whether linked to a paraphilic desire or Somatoparaphrenia, which has been linked to damage to the posterior cerebral regions of the cortex, how can it be ethical to surgically remove body parts? We don’t affirm other mental health conditions, mental disorders or impairment or damage to the brain by ignoring medical ethics of FIRST DO NO HARM this way.
The work of Dr Money, WPATH and those associated with the removal of paraphilias from the DSM-V are deeply ideological and highly discredited, hugely in part to their UNETHICAL practices and experimental surgeries. Though I understand medicine has moved on through tests, trials, experiments and research. This cannot just be done “to see” if something works with blatant disregard for humanity and ethics around clinical trials. Peer reviewed work from ideological physicians with an agenda, not based on what may be empirically sound or in the patients best interests — is an abuse of power. When this kind of “research” or “experimental” treatment is advertised as “the answer” — when it is, in fact to serve their own ends — and NOT those of future patients, we must be brave enough to take a stand and challenge the “professionals”. If their practice and research is sound and ethical it will pass any tests of scrutiny. You do not require a medical degree to test the ethics of an experimental treatment.
REFERENCES:
Mia @_CryMiaRiver Ottawa, Ontario & Jen @JenKTeach England, UK
Billingham, M., Davenport, P., Talman, H., Matthews, N., Stretch, B. and Author. (2016).BTEC National Health and Social Care Student Book 1. Harlow, United Kingdom: Pearson Education Canada, p.14, Meeting Individual Care and Support Need.
Pranzarone,G. F. PhD Available online at: ApotemnophiliaaParaphiliaorBodyIntegrityIdentityDisorderBIID.DysphoriaResolvedbySelf-Amputation.CaseHistory12-YearFollow-upwithMedicalEthicalIssues.pdf Accessed on 13th February 2023.
Quora. (2016). What are the differences between consequentialism, deontology, and virtue ethics? Available online at:https://www.quora.com/What-are-the-differences-between-consequentialism-deontology -and-virtue-ethics Accessed on 17th October 2019.
^ Vallar G., Ronchi R. (2009). “Somatoparaphrenia: a body delusion. A review of the neuropsychological literature”. Experimental Brain Research. 192 (3): 533–551. doi:10.1007/s00221–008–1562-y. PMID18813916. S2CID206924931.
^ Coltheart M (2005). “Delusional belief”. Australian Journal of Psychology. 57 (2): 72. doi:10.1080/00049530500125082.
^ Vallar G., Ronchi R. (2009). “Somatoparaphrenia: A body delusion. A review of the neuropsychological literature”. Experimental Brain Research. 192 (3): 533–51. doi:10.1007/s00221–008–1562-y. PMID18813916. S2CID206924931.
^ Fotopoulou A., Jenkinson P.M., Tsakiris M., Haggard P., Rudd A., Kopelman M.D. (2011). “Mirror-view reverses somatopharaphrenia: Dissociation between first- and third-person perspectives on body ownership”. Neuropsychologia. 49 (14): 3946–3955. doi:10.1016/j.neuropsychologia.2011.10.011. PMID22023911. S2CID25892919.
Manage Cookie Consent
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behaviour or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.