
Introduction
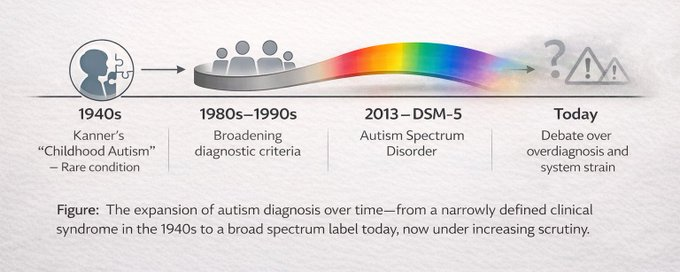
I was inspired to write this article after reading a piece in the Sunday Times: Six decades ago, autism was a little-known condition affecting perhaps 1 in 2,500 children, described in stark clinical terms as “childhood psychosis.” Today, recorded diagnoses have surged to around 1.3% of the UK population and roughly one in five English school pupils falls under the broader SEND (special educational needs and disabilities) umbrella, with autism and related neurodiversity labels driving much of the increase. Dame Uta Frith, one of the architects of the modern understanding of autism, now warns that the “spectrum” she once championed “has come to its collapse.” The label has been stretched so far that it no longer functions as a useful medical diagnosis.

A recent policy critique echoes this, asking bluntly: “What if there’s nothing wrong with the children?” and highlighting how diagnostic expansion, social media, and a neuro-affirmative approach risk medicalising ordinary variation while failing those with the greatest needs. This article traces autism’s conceptual journey from its origins to the present crisis. Drawing on peer-reviewed studies, NHS data, government reports and expert voices (including Frith and former Ofsted chief Baroness Amanda Spielman), it shows that the dramatic rise in diagnoses reflects broadened criteria and heightened awareness far more than any true increase in prevalence. The current “spectrum” has become scientifically noisy, clinically unhelpful and fiscally unsustainable. Subgroups, not an infinitely elastic label, offer a clearer path forward.
Historical Origins: A Narrow, Severe Neurodevelopmental Condition (1940s–1970s)
The modern concept of autism as a distinct disorder began in 1943 when Leo Kanner described 11 children with “autistic disturbances of affective contact”; profound social withdrawal, language impairment, repetitive behaviours, and early onset. He emphasised two essential features of the condition:
- (1) autism—or severe problems in social interaction and connectedness from the beginning of life, and
- (2) resistance to change/insistence on sameness.
The latter term also included some of the unusual stereotyped movements he noted such as body rocking and hand flapping. To Kanner, these movements appeared to be ways for the child to maintain sameness in his or her world.
Hans Asperger independently described similar but higher-functioning children in 1944, he defined autism as a rare, lifelong neurodevelopmental disorder. Unlike Kanner who emphasised the importance of autism as a developmental condition, Asperger described behaviours that more closely resembled a personality disorder and reported that fathers of his cases showed similar problems. Prior to this, behaviours were often folded into schizophrenia or “childhood psychosis.”
Until the 1970s, prevalence estimates hovered between 1 in 2,500 and 1 in 10,000. Behaviours were often misattributed to “refrigerator mothers” or schizophrenia. No spectrum existed; autism was binary and unmistakable. The term “autism” itself was coined by Eugen Bleuler in 1911 but referred to schizophrenic withdrawal. Diagnosis remained informal and extremely rare…
The Spectrum Concept Emerges: Inclusivity as Progress (1980s–1990s)
During the 1970s, there were important developments in the area of psychiatric diagnosis in general and in autism in particular that contributed to the decision to include autism as an official diagnostic category. Overall, there was increasing dissatisfaction with the chaotic state of affairs that had prevailed with psychiatric diagnoses in earlier versions of the APA’s manual. The DSM-III (1980) first gave autism its own category (“infantile autism”).
Lorna Wing’s 1981 paper popularised Asperger’s work in English and introduced the idea of a continuum and a “spectrum” of severity.
Uta Frith’s 1985 “theory of mind” studies (with Simon Baron-Cohen and Alan Leslie) provided a cognitive framework and explanation for social deficits and helped justify inclusion of verbally fluent, intelligent children who did not fit classic criteria, the milder “not-so-typical” cases.
The DSM-IV (1994) formalised separate but related diagnoses: autistic disorder, Asperger’s syndrome and pervasive developmental disorder-not otherwise specified (PDD-NOS). This expansion captured previously excluded intelligent, verbal individuals and boosted research and services, it was widely viewed as humane progress.
DSM-5 and the Final Broadening (2013–Present)
The DSM-5 (2013) collapsed all subcategories into a single “autism spectrum disorder” (ASD) with two core domains (social communication and restricted/repetitive behaviours) and severity specifiers. The intent was to reduce diagnostic confusion. Instead, it accelerated inclusion of individuals with subtle or late-emerging traits. Diagnosis remained purely behavioural; there were no biomarkers were added. Traits once considered personality quirks (extreme social anxiety, sensory hypersensitivity, aversion to routine change) became eligible for the label, especially in adults and women.
This takes a step away from Learning disabilities and their classifications: A learning disability is a reduced intellectual ability and difficulty with everyday activities, with onset in childhood. NICE states that: ‘A learning disability is generally defined by three core criteria:
- Lower intellectual ability (usually an IQ of less than 70).
- Significant impairment of social or adaptive functioning.
- Onset in childhood.’
The WHO classifies severity of an intellectual disability as:
- Mild (0.1-2.3 percentile): approximate IQ range of 50 to 69 (in adults, mental age from 9 to under 12 years). Likely to result in some learning difficulties in school. Many adults will be able to work and maintain good social relationships and contribute to society.
- Moderate (0.003-0.1 percentile): approximate IQ range of 35 to 49 (in adults, mental age from 6 to under 9 years). Likely to result in marked developmental delays in childhood but most can learn to develop some degree of independence in self-care and acquire adequate communication and academic skills. Adults will need varying degrees of support to live and work in the community.
- Severe (below 0.003 percentile): approximate IQ range of 20 to 34 (in adults, mental age from 3 to under 6 years). Likely to result in continuous need of support.
- Profound ((below 0.003 percentile): IQ under 20 (in adults, mental age below 3 years). Results in severe limitation in self-care, continence, communication and mobility.
The Diagnosis Explosion: Numbers vs Reality
UK recorded diagnoses rose 787% from 1998 to 2018. NHS data shows that, in England, recorded autism diagnoses rose from ~0.1% of the population in 1998 to 1.33% by 2024. Meaning, that now 1.3% of the English population now carries an ASD label.
Among schoolchildren, over 1.7 million pupils (one in five) now have special educational needs support, with autism, ADHD, social-emotional difficulties and speech needs driving the milder end of the increase. Education, Health and Care Plans (EHCPs) have more than doubled in a decade. Parallel rises appear in the US mong 8-year-olds climbing from 1 in 150 (2000) to 1 in 36 (2020), similar surges occurred in Australia, Sweden, and elsewhere. Crucially, the steepest growth is among later-diagnosed, verbally fluent adults and adolescents; especially women, while severe early-childhood cases with intellectual disability have remained stable. Active screening studies (e.g., Adult Psychiatric Morbidity Survey 2007–2023/24) show stable true prevalence (0.8–1.0% in adults) when the entire population is assessed rather than relying on clinical referrals.
Why the Rise Is Mostly Artefactual: Expanded Criteria and Awareness, Not a True Epidemic
The dramatic increase in recorded autism diagnoses over recent decades; such as the 787% rise in the UK from 1998 to 2018, is largely artefactual, meaning it stems from changes in how we identify, define, and report the condition rather than a genuine surge in the underlying prevalence of autism spectrum disorder (ASD). Multiple large-scale, population-based studies consistently support this conclusion. A key UK cohort study using Clinical Practice Research Datalink (CPRD) data from 1998–2018 documented this exponential 787% increase in recorded diagnoses. Researchers attributed the vast majority of this rise to broadened diagnostic criteria (particularly following DSM-IV in 1994 and DSM-5 in 2013), diagnostic substitution (where children once labelled with intellectual disability, language disorders, or other conditions are now classified under ASD), and heightened awareness among clinicians, educators, and parents. Similar patterns emerge from US CDC Autism and Developmental Disabilities Monitoring (ADDM) Network reports and Danish national registry analyses, which estimate that 60–90% of observed increases result from shifts in diagnostic practices, routine screening, service incentives, and reduced stigma around neurodevelopmental labels.
Crucially, evidence from active population screening shows that true underlying prevalence has remained stable. The UK’s Adult Psychiatric Morbidity Survey (APMS), which uses rigorous clinical assessments (including the Autism Diagnostic Observation Schedule, ADOS), found autism prevalence in adults hovering around 0.8–1.0% across surveys in 2007, 2014, and 2023/24; with no significant change over time. This stability in screened general-population samples contrasts sharply with the steep climb in clinical referrals and recorded diagnoses, reinforcing that better detection and wider criteria explain most of the apparent “epidemic.”
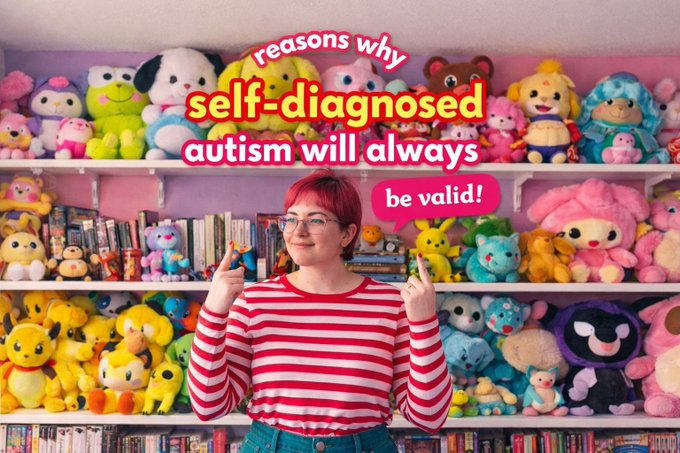
Social media has further accelerated the trend, particularly through self- and parent-driven diagnoses. Platforms like TikTok have amplified relatable but often oversimplified or inaccurate portrayals of neurodivergence; for instance, videos under #ADHD (closely related in overlap with autism discussions) have amassed billions of views (with top content frequently containing misinformation or normalising everyday experiences as diagnostic traits). Clinicians increasingly report adolescents and young adults presenting with self-derived labels from online sources, contributing to higher identification rates among milder, later-onset presentations; especially in women and verbally fluent individuals, without a proportional rise in severe, early-onset cases involving intellectual disability or profound communication impairments.
“Baroness Spielman, who ran Ofsted from 2017 to 2023, warned in a Sunday Times interview last September, that schools have reconceived themselves as therapeutic institutions, and that when they look for things wrong with children, they’ll probably find them. The risk here is creating a negative spiral that encourages children to understand ordinary adolescent difficulties as disorders.”
In summary, triangulated evidence from cohort studies, registry data, and population surveys attributes the increase primarily to: Broadened criteria in successive DSM editions, which now capture “high-functioning,” adult-onset, and subtler presentations previously excluded.
These non-biological factors explain 60–90% (and often more) of the documented rise across independent sources. No corresponding “biological epidemic”, such as environmental toxins, genetic shifts, or other causal agents, aligns with the data pattern, as severe forms of autism have not increased proportionally. The rise reflects improved recognition and an expanded conceptual net, not a sudden proliferation of the condition itself.
The Current State: Why the Label Has Become Unhelpful
The single “autism spectrum disorder” (ASD) label, as currently defined, has lost much of its clinical and scientific utility due to extreme heterogeneity. It now encompasses an extraordinarily wide range: from profoundly non-verbal individuals with severe intellectual disability who require lifelong, intensive care to verbally fluent, high-IQ adults whose primary challenges involve social anxiety, sensory hypersensitivity, or discomfort with change; traits that were once often viewed as personality variations or subclinical sensitivities rather than core neurodevelopmental pathology. This lack of a unifying biological or cognitive thread across the spectrum creates fundamental problems. No single genetic marker, brain anomaly, or neuropsychological profile reliably characterises all diagnosed individuals, complicating efforts to identify consistent underlying mechanisms.
As a result, research data become increasingly “noisy”: pooling such heterogeneous groups dilutes potential signals, hinders the discovery of reliable biomarkers, and undermines the replicability of findings in treatment trials and etiological studies. Experts have noted that this diagnostic inclusivity; while well-intentioned, has contributed to a form of “self-inflicted” heterogeneity that biases results toward false negatives and stalls progress that was more evident when research focused on more prototypical presentations.
Resource allocation suffers acutely from this over-inclusivity. NHS data show that open referrals for suspected autism have ballooned dramatically: as of December 2025, over 254,000 patients in England were waiting for assessment, with the vast majority (around 90%) exceeding the recommended 13-week guideline. Milder, later-diagnosed cases; often driven by self-referral or heightened awareness, overwhelm diagnostic pathways and support services, leaving those with profound needs (e.g., severe intellectual disability and communication impairments) facing even longer delays and inadequate provision. Cultural and social dynamics exacerbate the issue. The neurodiversity movement, popular media portrayals (e.g., “autistic-coded” TV characters), and online communities have, for some, turned an ASD diagnosis into a desirable identity marker or explanation for everyday struggles. This glamorisation and self-diagnosis trend contrasts sharply with the lived reality of many with high-support needs, who report feeling eclipsed or marginalised as attention and resources shift toward milder presentations. In contrast, conditions like general learning disability (intellectual disability; IQ typically <70 with adaptive impairments from childhood) remain more narrowly defined and often co-occur with autism (increasing risks of challenging behaviour and complex needs), yet require distinct support pathways focused on severe/profound levels.
Meanwhile, over-inclusive labelling risks medicalising normal human variation; such as introversion, sensory preferences, or transient anxiety, potentially leading to unnecessary pathologisation. It can also delay accurate identification and treatment of co-occurring or alternative conditions (e.g., primary anxiety disorders, ADHD, trauma-related issues, or other psychiatric presentations) by prematurely attributing symptoms to autism.
In essence, the current all-encompassing spectrum has blurred diagnostic boundaries to the point where the label no longer reliably guides clinical decision-making, advances scientific understanding, or equitably distributes finite resources. This state of affairs risks undermining public trust in the diagnosis and, ultimately, harms the very individuals the framework was intended to support.
Policy Implications: The UK SEND Reforms and Unasked Questions
The 2026 Schools White Paper “Every Child Achieving and Thriving” acknowledges the 1.7 million SEND figure but remains silent on diagnostic expansion, social media contagion, or the convergence with gender identity (meta-analyses show ~11% of transgender youth are autistic; roughly ten times population rate). It takes evidence almost exclusively from “neuro-affirmative” sources and proposes more identification, more specialists and more funding; precisely the opposite of calls for restraint from Frith, Spielman and others. It also overlooks persistent overlaps with intellectual/learning disability, where 20–30% of those with learning disability have co-occurring autism, amplifying needs for targeted health checks and behavioural support without conflating the conditions. Without interrogating root causes, the £4 billion+ settlement risks instability and backlash that could ultimately harm the most severely affected children.
Voices for Reform: Subgroups Over Spectrum
Dame Uta Frith, emeritus professor at UCL’s Institute of Cognitive Neuroscience and a foundational figure in autism research, has been instrumental in shaping the modern understanding of autism. She argues that the label has become “completely meaningless” as a medical diagnosis, encompassing such diverse presentations that it no longer guides effective research, treatment, or support. Frith emphasises that “there is no longer something that unites all the people who are diagnosed as autistic,” and she no longer believes in a single spectrum. To restore precision and clinical utility, Frith proposes replacing the broad spectrum with meaningful subgroups, each potentially with its own distinct label. She identifies at least two major subgroups:
- Classic childhood autism: Individuals diagnosed in early childhood (typically before age 3–5), often with significant intellectual disability (ID), language impairment, and profound social-communication challenges. These cases frequently involve behaviours that are challenging and require intensive, lifelong support. Frith argues this group aligns most closely with the original clinical descriptions (e.g., Kanner’s autism) and should retain the core “autism” label.
- Later-diagnosed group (often termed “hypersensitivity” or similar): Predominantly adolescents and young adults, especially women, diagnosed much later in life. These individuals are verbally fluent, without intellectual impairment, and capable of verbal and non-verbal communication, but they experience high social anxiety, hypersensitivity (e.g., to sensory input or change), and difficulties in social situations. Frith acknowledges these problems as real and deserving of support, but contends they may be better addressed under alternative or separate labels (e.g., anxiety-related or hypersensitivity conditions) rather than autism, as the autism framework can hinder targeted interventions.
- Frith also references a third potential category echoing historical distinctions: Asperger-type presentations; High-functioning individuals with early social differences, good language, and no intellectual disability (formerly Asperger’s syndrome before DSM-5 consolidation). She suggests clear distinctions like these would help tailor classroom support, research focus, and resources more effectively; for instance, recognising that early-diagnosed children with ID often need structured behavioural interventions, while later-diagnosed adolescents may benefit more from anxiety management or social skills training.
Beyond Frith’s proposals, other researchers have long advocated for moving away from a monolithic spectrum toward more nuanced frameworks:
- Dimensional approaches: Viewing autism traits (social-communication deficits, restricted/repetitive behaviours) as lying on continuous dimensions of severity rather than categorical presence/absence. This allows for heterogeneity without forcing artificial subgroups, supported by studies showing symptom distributions in toddlers and children align more with severity gradients than discrete types.
- Splitting by key moderators: Subtyping based on presence or absence of intellectual disability and language level. Cluster analyses have identified consistent patterns: one subgroup with severe impairments across domains (including ID and minimal language), another with moderate social-communication issues but fewer repetitive behaviours, and a third with milder overall symptoms but prominent restricted interests. Such divisions improve predictive validity for outcomes, co-occurring conditions, and intervention response.
- Additional proposals: Some suggest incorporating developmental trajectories (e.g., stable vs. regressive onset), biological markers (when available), or co-occurring features (e.g., ADHD-like profiles) to refine subgroups further.
The overarching goal across these voices is precision without exclusion. Reformers argue that abandoning an infinitely stretchable spectrum would reduce research “noise,” enable better biomarker discovery, allocate scarce resources (e.g., NHS assessments, EHCPs) more equitably, and avoid over-pathologising milder traits while ensuring robust support for those with profound needs. Frith stresses this is not about denying help to anyone experiencing distress but about creating scientifically and clinically meaningful categories that better reflect reality. As debates continue; with some autistic advocates and experts critiquing Frith’s views as out of touch with “lived experience”; the push for subgroups represents a call to evolve the field toward greater accuracy and fairness.
Summary of the Article “Autism study is my life’s work. The spectrum has lost all meaning” by Dame Uta Frith

The Sunday Times piece (7th March 2026) profiles Dame Uta Frith, emeritus professor at UCL’s Institute of Cognitive Neuroscience and a foundational figure in autism research since 1966. She helped establish the “theory of mind” deficit and championed the spectrum concept in the 1980s (building on Lorna Wing’s work), and now argues the autism spectrum has “come to its collapse.” She contends that extreme inclusivity has eliminated any common denominator for ASD diagnoses, stretching the label to encompass everything from profound childhood impairments to mild adult social anxiety or hypersensitivity; rendering it “meaningless” as a medical diagnosis.
Key points include: NHS-recorded autism diagnoses in England rose from ~0.1% (1998) to 1.33% (2024), driven almost entirely by later-diagnosed, verbally fluent, non-intellectually-disabled individuals (especially women). Severe, early-onset cases with intellectual disability have remained stable. No biomarkers exist, so diagnosis is purely behavioural and now includes traits once viewed as personality quirks.
Conclusion: Time to Rethink, Not Abandon
Autism as a concept has evolved from a rare, devastating syndrome to a catch-all that serves no one well. The evidence is clear: the dramatic rise in diagnoses reflects expanded criteria and awareness far more than a true increase in cases. Retaining a single, infinitely stretchable “spectrum” undermines science, strains services, and risks harming the very people it was meant to help. A return to meaningful, evidence-based subgroups; combined with continued support for all who struggle, offers a humane and scientifically rigorous path forward. The field Frith helped build now requires her courage to evolve again. The children and families who truly need help deserve nothing less.
Reference List
- American Psychiatric Association (1980) Diagnostic and statistical manual of mental disorders (3rd edn) (DSM-III). Washington, DC: American Psychiatric Association.
- American Psychiatric Association (1994) Diagnostic and statistical manual of mental disorders (4th edn) (DSM-IV). Washington, DC: American Psychiatric Association.
- American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders (5th edn) (DSM-5). Arlington, VA: American Psychiatric Publishing.
- BBC News (2026) What is SEND and how many children get support? 23 February. Available at: https://www.bbc.com/news/articles/cwy18y5jpw1o (Accessed: 8 March 2026).
- Biomarker reviews: Frye et al. (2019), Klin et al. (2018), Cortese et al. (2025). pmc.ncbi.nlm.nih.gov
- Castro, K. et al. (2026) ‘Autism spectrum disorder: overdiagnosis or a new pandemic?’, Jornal de Pediatria, [online]. Available at: https://www.sciencedirect.com/science/article/pii/S0021755725001299 (Accessed: 8 March 2026).
- CDC ADDM Network reports (2000–2022); meta-analyses on diagnostic substitution (e.g., Scientific American 2025 summary). scientificamerican.com
- Department for Education (2026a) Neurodivergence Task and Finish Group: report. London: Department for Education. Available at: https://www.gov.uk/government/publications/neurodivergence-task-and-finish-group-report (Accessed: 8 March 2026).
- Department for Education (2026b) Special educational needs in England, Academic year 2024/25. Available at: https://explore-education-statistics.service.gov.uk/find-statistics/special-educational-needs-in-england/2024-25 (Accessed: 8 March 2026).
- Frith, U. (2026) Interviews in TES Magazine and The Sunday Times (March). tes.com https://www.thetimes.com/uk/healthcare/article/autism-is-my-lifes-work-the-spectrum-has-become-meaningless-lg366z0wj
- Kanner, L. (1943) ‘Autistic disturbances of affective contact’, Nervous Child, 2, pp. 217–250.
- Litman, A. et al. (2025) ‘Decomposition of phenotypic heterogeneity in autism reveals underlying genetic programs’, Nature Genetics, 57, pp. 1611–1619. doi: 10.1038/s41588-025-02224-z.
- NHS Digital (2025) Autism statistics and Adult Psychiatric Morbidity Survey 2023/24. Available at: https://digital.nhs.uk/data-and-information/publications/statistical/autism-statistics (Accessed: 8 March 2026).
- NHS England Digital (2026) Autism Statistics, January 2025 to December 2025. Available at: https://digital.nhs.uk/data-and-information/publications/statistical/autism-statistics/january-2025-to-december-2025 (Accessed: 8 March 2026).
- Patient.info (2022) General learning disability. Available at: https://patient.info/doctor/paediatrics/general-learning-disability (Accessed: 8 March 2026).
- Right Wing Woman (2026) ‘What if there’s nothing wrong with the children?’, Right Wing Woman Substack, 8 March. Available at: https://rightwingwoman.substack.com/p/what-if-theres-nothing-wrong-with (Accessed: 8 March 2026).
- Rosen, N. E., Lord, C. and Volkmar, F. R. (2021) ‘The diagnosis of autism: from Kanner to DSM-III to DSM-5 and beyond’, Journal of Autism and Developmental Disorders, 51(12), pp. 4253–4270. doi: 10.1007/s10803-021-04904-1. https://doi.org/10.1007/s10803-021-04904-1
- Russell, G. et al. (2022) ‘Time trends in autism diagnosis over 20 years: a UK population-based cohort study’, Journal of Child Psychology and Psychiatry, 63(6), pp. 674–682. doi: 10.1111/jcpp.13505. pubmed.ncbi.nlm.nih.gov
- Spielman, A. (2025–2026) Statements at Policy Exchange events and Lords debates, reported in TES, The Spectator and The Sun.
- The Telegraph (2026) ‘Autism spectrum now so inclusive it is meaningless, says expert’, 5 March. Available at: https://www.telegraph.co.uk/news/2026/03/05/no-autism-spectrum-expert-pioneered-concept-says (Accessed: 8 March 2026).
- Tollit, M. A. et al. (2024) ‘A comparison of gender diversity in transgender young people with and without autistic traits’, PMC. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC11127512/ (Accessed: 8 March 2026).
- Wing, L. (1981) ‘Asperger’s syndrome: a clinical account’, Psychological Medicine, 11(1), pp. 115–129.
- All sources accessed or verified as of 8 March 2026. Data triangulated across NHS, government statistics, peer-reviewed meta-analyses and direct policy documents.