


Eating disorders are serious mental health conditions that affect millions worldwide, often using food and body image as mechanisms to cope with deeper emotional distress. In the UK, organisations like Beat Eating Disorders lead initiatives such as Eating Disorders Awareness Week (EDAW), which in 2026 runs from 23rd February to 1st March under the theme of “Community”. This week highlights the isolating nature of these disorders while emphasising the role of support networks, including online communities, in recovery.
https://edaw.beateatingdisorders.org.uk
EDAW encourages sharing stories, fundraising, and education to combat stigma, with events like workshops on social media’s impact on eating disorders. Key messages stress that no one is alone, and early intervention can lead to full recovery. In the UK, eating disorders affect around 1.25 million people, with a quarter being male, and inequalities persist for minority ethnic groups, LGB individuals, and those from low socioeconomic backgrounds. Compared to the US, where lifetime prevalence is estimated at 2-5% and more common in females, or Canada, where similar patterns emerge, the UK focuses on integrated NHS services for detection and treatment.
This article explores all types of eating disorders, their risks and treatments, while examining social media’s influence, the social contagion angle, and risks from assisted dying legislation, with a UK lens and international comparisons.
Types of Eating Disorders
Eating disorders manifest in various forms, often overlapping, and diagnoses can evolve. The UK’s NHS and Beat recognise several types, aligned with international classifications like those from the US’s National Institute of Mental Health (NIMH) or Cleveland Clinic. Below, each is described with risks and treatments, drawing from UK guidelines (e.g., NICE) and global evidence.
Anorexia Nervosa
Anorexia (or anorexia nervosa) is a serious mental illness that often causes individuals to limit how much they eat or drink. Some people develop strict “rules” about what, when, or where they can eat. This involves severe restriction of food intake, intense fear of weight gain, and distorted body image. In the UK, it’s the most studied, often linked to perfectionism or trauma. There are two main subtypes of anorexia nervosa:
- Restricting subtype (AN-R): Characterised by severe restriction of the amount and type of food they eat. Behaviours may include skipping meals, counting calories, and following rigid food rules.
- Binge–purge subtype (AN-BP): This also involves restriction, but people may also do lots of exercise, make themselves sick, or misuse laxatives to “get rid” of food eaten. They may also experience cycles of bingeing (eating large amounts of food at once whilst feeling out of control) and then purging. Sometimes AN-BP can be confused with bulimia nervosa. However, the main difference is that people with AN-BP continue to restrict their intake overall and are typically underweight, whereas people with bulimia nervosa are usually within or above what is considered a healthy weight range. Both are serious and deserving of support.
Anorexia can cause severe physical problems because of the effects of starvation on the body. It can lead to loss of muscle strength and reduced bone strength. Girls and women may find that their periods stop, which is known as ‘amenorrhoea’. They may also find that their sex drive decreases.
As with other eating disorders, anorexia can be associated with depression, low self-esteem, anxiety, and other complications and comorbidities. Risks include malnutrition, heart arrhythmias, erosion of tooth enamel, osteoporosis, difficulty conceiving, infertility, damage to other organs, such as the kidneys, bowels and liver, weakened immune system, delayed onset of puberty or stunted growth in children and young teenagers and fatality, there is a high mortality (standardised mortality ratio reduced from 11.2 to 2.9 in Denmark with specialised care).
Treatments: Family-based therapy for adolescents; cognitive behavioural therapy (CBT), Maudsley Model for Adults (MANTRA), Specialist supportive Clinical Management (SSCM), or focal psychodynamic therapy for adults. In the US and Canada, similar therapies are used, but access varies; Lisdexamfetamine (Vyvanse, Elvanse) is a central nervous system stimulant used primarily to treat Attention Deficit Hyperactivity Disorder (ADHD) in children (6+) and adults, as well as moderate to severe binge eating disorder (BED) in adults, and is approved in North America for related binge eating.
Bulimia Nervosa
Bulimia nervosa (commonly known as bulimia) is a serious mental health condition and eating disorder. It can impact people of any age, gender, ethnicity, or background. Individuals with bulimia often become trapped in a repeating cycle of binge eating; consuming unusually large amounts of food in a short period, followed by attempts to “undo” the overeating through compensatory behaviours (known as purging). These may include self-induced vomiting, misusing laxatives or diuretics, fasting, or excessive exercise. In the UK, bulimia and other eating disorders tend to be more prevalent among young adults and adolescents, with recent data showing notably higher rates in those aged 17–25 compared to younger teens or older groups. Binge eating episodes are frequently triggered as a way to manage overwhelming or negative emotions, such as stress, sadness, anger, or anxiety. During a binge, the person typically feels a profound loss of control over both the quantity of food consumed and the speed of eating.
People with bulimia are often a “normal” weight and hide their illness from others, it can be very difficult to spot from the outside. Often they are reluctant to seek help. As with other eating disorders, people around a person with bulimia will probably notice changes to their mood and feelings before seeing any physical change.
Bulimia can cause serious damage to the body. Long-term effects of bulimia include: Permanent damage to teeth, damage to the vocal chords and throat, damage to the intestines and stomach, electrolyte imbalances, increased risk of heart problems, kidney damage and co-occurring depression. If left untreated, bulimia nervosa can cause long-term harm to the body and may even be fatal. However, many physical effects of bulimia are reversible or can be prevented from worsening with the right treatment, and eating disorders are treatable, with full recovery possible.
Treatments: Therapy can be recommended as part of the treatment for bulimia in order to tackle the underlying thoughts and feelings that cause the illness and encourage healthier ways of coping. Guided self-help or CBT; For adults, NICE recommends guided self-help focused on bulimia. This should use self-help materials based on CBT, and should involve supportive sessions over the course of the programme to help ensure its effectiveness. stepped-care models in Finland showed cost-effective quality-of-life improvements. US RCTs confirm stepped care’s superiority over usual care. For children and young people, NICE recommends family therapy focused on bulimia. If this is unacceptable or ineffective it recommends individual CBT focused on eating disorders.
Binge Eating Disorder (BED)
Binge eating disorder (BED) is a serious eating disorder characterised by recurrent episodes of consuming unusually large amounts of food in a short time, during which the person feels a significant loss of control over their eating. It can affect anyone, regardless of age, gender, ethnicity, or background. Research indicates that BED is the most common eating disorder in the UK, with estimates suggesting it affects around 1 in 50 people (approximately 2% of the population), and it is more prevalent than disorders like anorexia or bulimia. Many cases remain underdiagnosed and untreated. Unlike bulimia, BED does not involve regular compensatory behaviours such as vomiting, misusing laxatives, or excessive exercise to “undo” the binge. However, individuals may occasionally fast or restrict between binge episodes. BED is not simply overindulging or choosing large portions, binges are highly distressing and typically involve eating far more food than intended, often to the point of discomfort. People frequently describe feeling unable to stop eating during an episode, even when they want to. Many report a sense of disconnection or dissociation during the binge, and some struggle to recall exactly what or how much they ate afterward. Episodes can be planned (e.g., like a ritual, involving purchasing specific “binge foods”) or spontaneous. In severe cases, individuals may go to great lengths to obtain food, such as eating discarded items or food that isn’t theirs. Binges almost always occur in secret or privately, even though the person may eat normal meals at other times. The distress, shame, and emotional turmoil associated with BED often lead to secrecy, guilt, and further emotional challenges, making professional support essential for recovery.
Binge eating disorder (BED), like other eating disorders, can lead to serious and potentially long-lasting physical health consequences, some of which may become permanent if the condition goes untreated for a prolonged period. Common long-term physical risks and complications associated with BED include: Obesity or significant weight gain, high blood pressure (hypertension), high cholesterol levels, heart disease (including increased risk of cardiovascular problems), Type 2 diabetes, Gallbladder disease, joint problems, back pain, or arthritis, Sleep apnoea or other breathing difficulties during sleep, Gastrointestinal issues, such as damage to the oesophagus, stomach problems, or conditions like gastroesophageal reflux disease (GERD), infertility or difficulties conceiving. In severe, untreated cases, these complications can become life-threatening, making BED potentially fatal without timely intervention. Importantly, many of these physical effects are reversible, can be prevented from progressing, or managed effectively with appropriate treatment.
Treatments: Eating disorders, including BED, are treatable mental health conditions, and full recovery is possible for many people. Beyond physical health, BED often has a profound impact on overall well-being and daily life. While not everyone with BED experiences obesity, weight gain is common and can contribute to the health risks listed above. Emotionally and psychologically, BED is strongly linked to low self-esteem, reduced confidence, depression, anxiety, feelings of shame, guilt, or disgust after episodes, and social withdrawal or isolation. Early recognition and support can make a significant difference in preventing escalation and promoting recovery. For adults with binge eating disorder, it recommends CBT or interpersonal psychotherapy as first-line therapies. If these are unsuitable, ineffective or inappropriate it says other treatment options could be considered, such as dialectical-based therapy, integrative cognitive-affective therapy, brief strategic therapy or schema therapy, or self-help; lisdexamfetamine in North America. The weight gain that binge eating disorder can cause is a symptom, not the illness itself. Both NICE and SIGN guidelines state that psychological therapies for BED do not aim to result in or focus on weight loss.
Avoidant/Restrictive Food Intake Disorder (ARFID)
Avoidant/restrictive food intake disorder (ARFID) is a recognised eating disorder where individuals severely limit or avoid certain foods or entire food groups, or restrict the overall amount they eat, or experience both. It can affect people of any age, from young children to adults, and occurs across all genders, ethnicities, and backgrounds. Unlike disorders such as anorexia nervosa, ARFID is not necessarily driven by concerns about body weight, shape, or appearance. Weight loss or low body weight may occur in some cases but is not required for diagnosis; ARFID can present at any weight. The avoidance or restriction typically stems from one or more of the following key factors:
- Sensory sensitivities: extreme aversion to the taste, texture, smell, appearance, or temperature of foods. For example, someone might only tolerate “safe” foods that are crunchy, bland, or a specific colour/brand, leading to a very narrow diet and sensory-based restriction.
- Fear of aversive consequences: intense anxiety or phobia related to eating, often triggered by a past traumatic experience (such as choking, vomiting, or severe abdominal pain). This can cause avoidance of foods perceived as risky, or general worries about what might happen after eating (e.g., choking, getting sick), even if hard to articulate. Significant fear can result in sticking only to “safe” foods.
- Lack of interest in eating or low appetite: some people may not recognise hunger cues in the same way others do, have generally poor appetite, or view eating as a burdensome chore rather than something enjoyable. This can lead to consistently low intake without strong sensory or fear-based triggers.
Many cases in the UK appear to originate from or become noticeable in childhood, though the condition can persist or emerge later. ARFID is increasingly recognised, with calls to eating disorder helplines like Beat rising significantly in recent years (from around 2% of inquiries in 2018 to about 10% more recently). While exact UK prevalence is not fully established and often underdiagnosed (sometimes mistaken for “picky eating”), estimates suggest it accounts for roughly 5% of eating disorder cases in some studies, with broader population screening indicating ARFID symptoms may affect a notable minority; potentially higher in certain groups like those with neurodevelopmental conditions (e.g., autism) or anxiety.
ARFID can lead to serious nutritional deficiencies, growth issues in children, or other health complications if untreated, such as growth delays, as well as a negative impact on their psychological wellbeing. Like other eating disorders, it is treatable with appropriate support, and recovery is achievable. Early identification and intervention are key.
Treatments: typically involve a multidisciplinary approach tailored to the individual’s specific triggers (such as sensory sensitivities, fear of aversive consequences, or lack of interest in eating), age, and severity of restriction. The primary focus is on behavioural therapies and psychological interventions, including: Cognitive behavioural therapy (CBT), including adapted forms like CBT-AR (CBT for ARFID), which helps address avoidance patterns, expand food variety, and reduce anxiety around eating. Behavioural interventions, such as gradual exposure work (systematically introducing feared or avoided foods in a supported way). Family-based treatment (especially effective for children and young people), where parents/carers play a key role in supporting consistent, structured mealtimes and encouraging progress. Anxiety management training and other strategies to build coping skills. In the UK, ARFID treatment is not yet covered by specific NICE or SIGN guidelines for eating disorders (unlike anorexia or bulimia), so access and approaches can vary by region and service. Individuals may be referred to specialist eating disorder services (for children/young people via CAMHS or community teams; for adults via specialist ED services or general mental health support), paediatric services, dietitians, speech and language therapists, occupational therapists, or psychologists. For individuals with very limited intake or significant nutritional/medical risk: Nutritional supplements (oral high-calorie drinks or formulas) are commonly prescribed to bridge gaps, a temporary period of tube feeding (enteral nutrition, such as nasogastric or gastrostomy) may be recommended to safely stabilise health while psychological and behavioural work continues. This is typically short-term and aimed at transitioning back to oral eating.
Other Specified Feeding or Eating Disorder (OSFED)
Anorexia, bulimia, and binge eating disorder are diagnosed using a list of expected behavioural, psychological, and physical symptoms. Sometimes a person’s symptoms don’t exactly fit the expected symptoms for any of these eating disorders. In that case, they might be diagnosed with an “other specified feeding or eating disorder” (OSFED). This is very common. OSFED accounts for the highest percentage of eating disorders. Less commonly nowadays, you might also hear the term “eating disorder not otherwise specified” (EDNOS) to refer to eating disorders that don’t fit all the expected symptoms of anorexia, bulimia, or binge eating disorder. EDNOS was used in the Diagnostic and Statistical Manual of Mental Disorders (DSM) classification system, which describes different types of eating disorders, from 1987 to 2013. In 2013 this was replaced by the current edition of the DSM, with some major changes to the section on eating disorders. Some specific examples of OSFED include:
- Atypical anorexia – where someone has all the symptoms a doctor looks for to diagnose anorexia, except their weight remains within or above the “normal” range.
- Bulimia nervosa (of low frequency and/or limited duration) – where someone has all of the symptoms of bulimia, except the binge/purge cycles don’t happen as often or over as long a period of time as doctors would use to diagnose bulimia.
- Binge eating disorder (of low frequency and/or limited duration) – where someone has all of the symptoms of binge eating disorder, except the binges don’t happen as often or over as long a period of time as doctors would use to diagnose binge eating disorder.
- Purging disorder – where someone purges, for example by being sick or using laxatives, to affect their weight or shape, but this isn’t as part of binge/purge cycles.
- Night eating syndrome – where someone repeatedly eats at night, either after waking up from sleep, or by eating a lot of food after their evening meal.
People with OSFED may work to hide their illness and someone may have been ill for a long time before physical symptoms appear, if they do at all. Risks and treatments mirror similar disorders (e.g., CBT-based). Self-help and support groups.
Pica
Pica is a feeding disorder in which someone eats non-food substances that have no nutritional value, such as paper, soap, paint, chalk, or ice. For a diagnosis of pica, the behaviour must:
- Be present for at least one month
- Not part of a cultural practice, and
- Be developmentally inappropriate e.g., it’s not generally diagnosed in children under the age of two, as it is common for babies to “mouth” objects, which can lead to them accidentally eating substances that aren’t meant to be eaten.
Often, pica is not revealed until medical consequences occur, such as metal toxicity, cracked teeth, or infections. It is more likely to first appear among children. It can occur alongside other illnesses, including other eating disorders. Rare in UK adults. People with pica don’t usually avoid regular food, meaning they may still be getting all the nutrients they need. However, some non-food items eaten can be very dangerous, especially if eaten in large amounts. It has been linked with iron or ferritin deficiency. In some people, pica behaviours improve once these deficiencies are corrected. However, not everyone with pica is deficient in minerals and vitamins, and it’s unclear whether it causes the behaviour or the other way around. It may be more likely to occur alongside: Pregnancy, Iron deficiency anaemia, Autism, Intellectual developmental disorders, Depression, Obsessive-compulsive disorder and related disorders such as trichotillomania (hair-pulling) and excoriation disorder (skin-picking), Schizophrenia or other mental health conditions. Risks include Toxicity, and intestinal blockages.
Treatment depends on the individual needs, the severity, and the underlying cause of the behaviour: These may include:
- Addressing nutritional deficiencies i.e. through supplementation
- Behavioural therapies – this can include promoting self-soothing behaviour, redirecting attention, managing anxieties, and replacing pica items with similar, but safe, alternatives
- Medical intervention e.g., in instances where the behaviour has led to physical health problems
- Medication may also be offered
- Addressing underlying conditions e.g., OCD, depression, schizophrenia
There are currently no widely used screening tools designed specifically for pica. However, newer questionnaires such as the Pica, ARFID, and Rumination Disorder Interview (PARDI), are being explored for use.
Rumination Disorder
Rumination disorder is an illness that involves repetitive, habitual bringing up of food that might be partly digested. It often occurs effortlessly and painlessly, and is not associated with nausea or disgust. Rumination disorder can affect anyone at any age. The exact causes of rumination disorder are not known.
Possible signs of rumination disorder include: Vomiting food that has been partly digested on a regular basis, No obvious physical illness that causes this behaviour, Re-chewing and swallowing food that they’ve brought up, Hiding their behaviour, for example, by coughing or covering their mouth, Avoiding eating around others, Avoiding eating before socialising, Weight loss, Malnutrition, Not making expected weight gains, Straining and arching the back with the head held back, making sucking movements with their tongue, Appearance of finding the behaviour satisfying, Being hungry and irritable between instances of bringing up their food.
The number of people who have rumination disorder is unknown. Rumination disorder can lead to malnutrition, weight loss, dental erosions, and electrolyte disturbances if left untreated. It is therefore very important to contact your doctor as soon as possible if you’re worried about yourself or someone you know, and to ask to be referred to a specialist who can rule out other causes for the behaviour and discuss appropriate treatment, Potentially habit reversal training.
Orthorexia
Orthorexia (also known as orthorexia nervosa) is a term coined in 1997 by Dr. Steven Bratman, MD, to describe an unhealthy obsession with eating only “pure,” “clean,” or “healthy” foods. What counts as “pure” or “impure” can vary widely between individuals, often leading to rigid rules about food quality, preparation, or origin. Unlike typical healthy eating or dietary preferences, orthorexia involves using strict food rules to cope with negative emotions, gain a sense of control, or manage underlying distress; turning what starts as a pursuit of wellness into a source of significant anxiety and impairment. Orthorexia is not currently recognised as a distinct clinical diagnosis in major classification systems like the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders) or ICD-11 (International Classification of Diseases). If someone seeks medical help with these patterns, they would not receive an official diagnosis of “orthorexia.” Instead, clinicians might discuss the term informally while assessing for related conditions. In the UK and elsewhere, it is often viewed as falling under broader categories of disordered eating. Prevalence estimates for orthorexia vary widely due to the lack of standardized diagnostic tools and criteria; ranging from under 1% to around 7% in the general population, with much higher rates (up to 35–58%) reported in certain high-risk groups like healthcare professionals, athletes, nutrition/dietetics students, or those in wellness-focused fields. In the UK, it is increasingly discussed in eating disorder resources (e.g., by Beat), though it remains under-recognised and often underdiagnosed.
Because of the extreme restrictions, orthorexia can lead to serious physical health problems, including: Nutritional deficiencies from eliminating entire food groups or essential nutrients, Malnutrition, Low energy levels and fatigue, Digestive issues, and other complications similar to those seen in restrictive eating disorders.
All eating disorders are serious mental illnesses that warrant prompt intervention. Early treatment offers the best opportunity for full recovery and prevents worsening physical or psychological harm. Orthorexia shares notable overlaps with anorexia nervosa, particularly in restrictive behaviours and perfectionism around food. Treatment is not standardised specifically for orthorexia, but approaches commonly draw from those effective for related conditions like anorexia or obsessive-compulsive patterns; such as cognitive behavioural therapy (CBT), nutritional rehabilitation, addressing perfectionism and anxiety, and multidisciplinary support from therapists, dietitians, and doctors. Recovery is possible with appropriate, tailored help.
Type 1 Diabetes and Disordered Eating (T1DE)
‘T1DE’ (which stands for type 1 diabetes and disordered eating) to refer to the experience of having an eating disorder while living with type 1 diabetes. While ‘T1DE’ is not currently listed as a formal medical diagnosis, it is increasingly recognised, for example, in guidelines published on Managing Medical Emergencies in Eating Disorders. It has also been referred to as ‘diabulimia’ in the media, but T1DE is used by healthcare professionals to capture the different symptoms someone may experience. People living with T1DE may restrict their insulin to attempt to control their weight. People may also engage in other eating disorder behaviours, such as restricting their intake, over-exercising or by purging (for example, by vomiting or taking laxatives or diuretics).
For someone with type 1 diabetes, restricting insulin can be very dangerous. Other medical risk factors include the management of hypoglycaemia (or low blood sugar level), starvation, and other purging behaviours such as vomiting, laxative misuse and exercise.
Find support – If you or someone you know is living with type 1 diabetes and experiencing disordered eating, Breakthrough T1D has information, shared experiences and links to further support. Treatments will often follow a multi-disciplinary and multi-method approach.
General Risks of Eating Disorders
Eating disorders carry high risks, including physical (e.g., organ failure, infertility) and psychological (e.g., anxiety, suicide ideation). In the UK, delayed diagnosis exacerbates outcomes; mortality is among the highest for psychiatric illnesses. Globally, 2-5% lifetime prevalence correlates with gender disparities (more females), but social factors like media pressure amplify risks. In Canada, teens face intensified fears; US studies link to chronic conditions.
Treatments for Eating Disorders
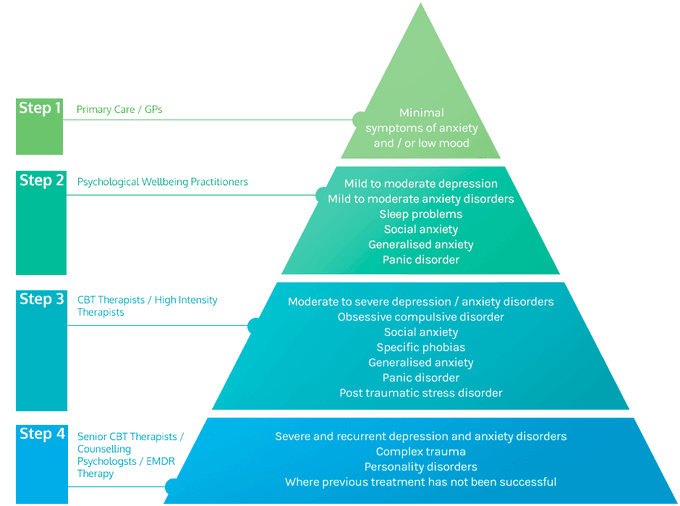
Recovery is possible with tailored interventions. UK NICE guidelines recommend specialist referral via GPs, with therapies like CBT or family therapy. Stepped-care models reduce costs (e.g., £12,146 vs. £20,317 per recovery in US studies). Emerging treatments include pharmacological options (e.g., off-label for AN). In Australia and the US, self-help shows mixed success; Canada emphasises family support. Co-occurring conditions require holistic care. The stepped care model is used by NHS Talking Therapies services to make a clinical decision as to which sort of treatment is currently the most appropriate for the person they are assessing.
The Impact of Social Media on Eating Disorders
Social media has reshaped narratives around eating disorders, often promoting harmful ideals. In the UK, EDAW addresses this through workshops on online safety. Multiple studies confirm that social media platforms contribute to reshaping perceptions of body image and eating disorders by promoting unrealistic ideals. For example, a 2023 scoping review of 50 studies across 17 countries found that social media usage leads to body image concerns and disordered eating through pathways like social comparison, internalisation of thin/fit ideals, and self-objectification. Platforms like TikTok, Instagram, Meta and X (formerly Twitter) expose users to “thinspiration” or “fitspiration” content, triggering body dissatisfaction. Studies show 51.7% of UK girls aged 13-14 report disordered behaviours after social media exposure. Pro-anorexia (pro-ana) and pro-bulimia (pro-mia) communities glamorise disorders, with algorithms reinforcing exposure. A 2021 New York Times investigation revealed TikTok recommending eating disorder-related videos to users as young as 13 within minutes of account creation. Discussions are growing around social media’s role in addiction crises, linking to anxiety and eating disorders. A 2025 SFU study found social media fuelling a “shadow pandemic” of disordered eating in teens, with 1-2 hours daily increasing risks. In the US, 86% want tech accountability; Canada notes peer influence via ads.
Social media offers recovery benefits through supportive forums. A 2020 study on Instagram recovery communities found users engage for motivation and connection, aiding recovery. Another 2020 analysis of ED-related forums identified themes of recovery as a psychosocial process, providing peer support. Positive aspects include recovery forums, but toxicity prevails on less moderated platforms.
The Social Contagion Angle
Social contagion theory suggests that behaviours can propagate through social networks, a phenomenon observed in eating disorders where peer influences facilitate the spread of disordered eating patterns. In the UK, research indicates clustering of these disorders within schools and peer groups, with studies showing higher diagnosis rates in institutions with greater proportions of female students or parents with higher education levels, potentially due to cultural pressures or imitation effects. For instance, a 2025 UK school-based study of over 7,400 adolescents revealed a 17% prevalence of probable eating disorders, with elevated risks among females (23.5%), and those from deprived areas, highlighting how social and environmental factors like body dissatisfaction exacerbate contagion. Peers often normalise behaviours such as bingeing or caloric restriction, while online platforms amplify pro-eating disorder (pro-ED) norms through communities that idolise anorexia as an identity or “lifestyle,” as noted by UK experts like Deanne Jade of the National Centre for Eating Disorders. These digital spaces show minimal interaction between pro-ED and recovery-oriented groups, reinforcing isolation.
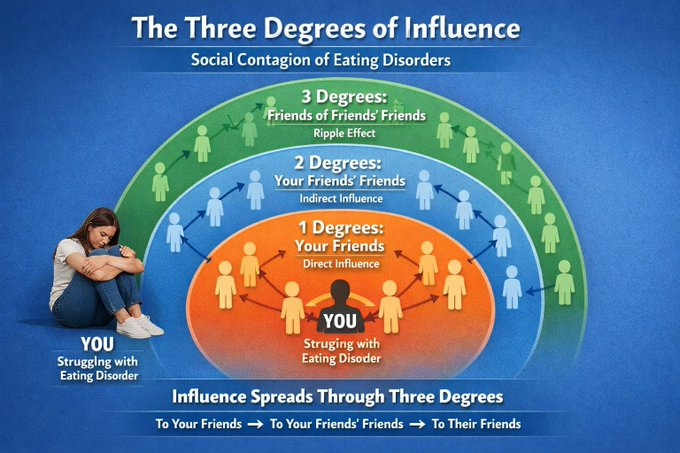
US data from high schools reports 4-10% clustering of symptoms like fasting and diet pill use. Globally, reviews combine contagion with dual-pathway models involving body dissatisfaction and dieting. Although critics highlight reverse causation, such as homophily (derived from Ancient Greek for “love of the same,” is the sociological tendency for individuals to associate and bond with similar others, often summarised as “birds of a feather flock together”) where similar individuals self-select into groups, frameworks like the three-degrees-of-influence rule demonstrate behavioural transmission across networks (In short, Christakis and Fowler posited that diverse phenomena “ripple through our network, having an impact on our friends (one degree), our friends’ friends (two degrees), and even our friends’ friends’ friends (three degrees). In Canada, similar dynamics connect to suicide clusters, while UK inpatient and residential settings pose risks of “peer contagion,” with reports of bullying and technique-sharing among patients.
Dangers of Assisted Dying Legislation and Eating Disorders
Assisted dying laws present profound risks for individuals with eating disorders, especially those with anorexia nervosa, where the condition can be misclassified as “irremediable” or terminal due to severe physical deterioration from self-starvation. This vulnerability arises because eating disorders often blur the lines between mental and physical health, potentially allowing patients to qualify for assisted death under criteria intended for terminal illnesses, even when their underlying condition is treatable with appropriate psychiatric intervention. In the UK, the Terminally Ill Adults (End of Life) Bill, which seeks to legalise assisted dying for adults with a prognosis of six months or less, has drawn sharp criticism for inherent loopholes that could enable access through voluntary or illness-driven refusal of food and fluids, despite explicit exclusions for mental disorders as the primary basis. For instance, critics argue that patients with anorexia could starve themselves to the point of organ failure, meeting the bill’s terminal illness definition without the mental health aspect being adequately addressed, thereby circumventing safeguards and leading to premature, preventable deaths among vulnerable groups, many of whom are young women in their teens or twenties.
Recent amendments debated in the House of Lords on February 6th, 2026, aimed to mitigate this by clarifying that physical decline resulting from mental illness-related restrictions on eating or drinking does not qualify someone as terminally ill, and further specifying that this applies regardless of whether the restriction is voluntary or compelled by the disorder. However, opponents, including eating disorder charities like Beat and Mind, contend that these changes fall short, as they fail to encompass other eating disorders such as bulimia or binge-eating disorder, where physical complications like electrolyte imbalances or heart failure could still be interpreted as terminal without robust mental health evaluations. This inadequacy is underscored by an open letter signed by media figures like Sophie Turner and Gail Porter, warning that the bill could render individuals with eating disorders eligible during periods of acute crisis when they cannot access or accept treatment, effectively prioritising death over recovery.
International evidence amplifies these concerns, revealing a pattern of exploitation in jurisdictions with similar laws. Between 2012 and 2024, at least 60 cases of euthanasia involving eating disorder patients; predominantly young women under 40, have been documented in the Netherlands, Belgium, and U.S. states like Oregon, where anorexia has been deemed a qualifying terminal condition despite its psychiatric roots. In Canada, the expansion of Medical Assistance in Dying (MAiD) to include sole mental illnesses starting in 2024 has heightened fears of a “slippery slope,” with reports of inadequate safeguards leading to approvals for patients whose eating disorders were compounded by treatable depression or trauma, resulting in deaths that could have been averted through better mental health support.
Such precedents highlight how initial restrictions erode over time, potentially normalising assisted death for non-terminal mental health conditions and pressuring vulnerable individuals during low points when suicidal ideation is prevalent; eating disorders already carry the highest mortality rate among psychiatric illnesses, often from suicide or medical complications, making this group particularly susceptible.
Perspectives on the issue vary widely: Proponents of the bill, including some peers like Lord Falconer, advocate for parity arguing that unbearable pain from any source warrants choice, and that amendments sufficiently protect against misuse by emphasising capacity assessments and excluding mental disorders as standalone qualifiers, though there is no mention of pain or suffering in the bill! They maintain that the UK’s framework, with requirements like two doctor approvals and judicial oversight, provides stronger barriers than international models.
Critics, including myself, the Royal College of Psychiatrists and survivors of anorexia, however, emphasise the inherent vulnerability of eating disorder patients, whose distorted body image and cognitive impairments can impair decision-making capacity, leading to coerced or impulsive requests for death amid societal pressures or inadequate treatment access. They point to the “slippery slope” evidenced abroad, where expansions have included adolescents and those with disabilities, and argue that the bill risks eugenics-like outcomes by devaluing lives affected by mental illness. In UK parliamentary debates, peers continue to push for stronger protections, such as explicit exclusions for any physical effects stemming from mental illnesses, while discussions amplify anorexia case studies, with users and experts decrying the bill as a moral catastrophe that could endanger the most fragile in society. Ultimately, the legislation could exacerbate existing inequalities in mental health care, turning what proponents call a “compassionate” intent into a pathway for avoidable tragedy among those battling eating disorders.
Conclusion: Towards Greater Awareness and Support
Eating disorders demand urgent awareness, especially during EDAW, to challenge harmful narratives amplified by social media and contagion. While UK services like NHS specialists offer hope, international comparisons reveal gaps in access and safeguards, particularly with assisted dying. Early intervention, community support, and policy reforms are key to recovery.

In the UK Beat’s free, confidential Helplines are here for you. Their Helpline page has more information about opening hours.
- England Helpline: 0808 801 0677 | help@beateatingdisorders.org.uk
- Scotland Helpline: 0808 801 0432 | Scotlandhelp@beateatingdisorders.org.uk
- Wales Helpline: 0808 801 0433 | Waleshelp@beateatingdisorders.org.uk
- Northern Ireland Helpline: 0808 801 0434 | NIhelp@beateatingdisorders.org.uk
You can also join one of their online support groups, which are anonymous and give you the opportunity to speak to people going through similar experiences to you. If you’d like to find face-to-face support in your area, you can use their HelpFinder service to see what’s available.
References
- AboutKidsHealth (2023) Avoidant/restrictive food intake disorder (ARFID): Treatment options. Available at: https://www.aboutkidshealth.ca/avoidantrestrictive-food-intake-disorder-arfid-treatment-options (Accessed: 23 February 2026).
- Allison, S., Warin, M. and Bastiampillai, T. (2014) ‘Anorexia nervosa and social contagion: Clinical implications’, Australian & New Zealand Journal of Psychiatry, 48(2), pp. 116–120.
- Babb, C. et al. (2022) ‘Investigating service users’ perspectives of eating disorder services: A meta‐synthesis’, Clinical Psychology & Psychotherapy, 29(1), pp. 2723-2737.
- Beat Eating Disorders (n.d.) ARFID – Avoidant/Restrictive Food Intake Disorder. Available at: https://www.beateatingdisorders.org.uk/get-information-and-support/about-eating-disorders/types/arfid (Accessed: 23 February 2026).
- Beat Eating Disorders (n.d.) How many people have an eating disorder in the UK? Available at: https://www.beateatingdisorders.org.uk/get-information-and-support/about-eating-disorders/how-many-people-eating-disorder-uk (Accessed: 23 February 2026).
- British Dietetic Association (n.d.) A Framework for Good Practice in Delivering Support to Adults and Older Adults with Avoidant Restrictive Food Intake Disorder (ARFID). Available at: https://www.bda.uk.com/asset/E205BF27-6C92-46C5-BE01DFB62AA97197 (Accessed: 23 February 2026).
- Bryson, C. (2024) ‘Established and emerging treatments for eating disorders’, Trends in Molecular Medicine, 30(1), pp. 34-45.
- Chung, A. et al. (2021) ‘Adolescent Peer Influence on Eating Behaviors via Social Media: Scoping Review’, Journal of Medical Internet Research, 23(6), e19697.
- Christakis, N.A. and Fowler, J.H. (2013) ‘Social contagion theory: examining dynamic social networks and human behavior’, Statistics in Medicine, 32(4), pp. 556–577.
- Cleveland Clinic (2024) Eating Disorders: What They Are, Symptoms, Treatment & Types. Available at: https://my.clevelandclinic.org/health/diseases/4152-eating-disorders (Accessed: 23 February 2026).
- Coelho, R. et al. (2023) ‘The realities of medical assistance in dying in Canada’, Palliative & Supportive Care, 21(5), pp. 871–878.
- Commission on Assisted Dying (2012) The current legal status of assisted dying is inadequate. Available at: https://demos.co.uk/wp-content/uploads/2012/01/476_CoAD_FinalReport_158x240_I_web_single-NEW_.pdf (Accessed: 23 February 2026).
- Crandall, C.S. (1988) ‘Social contagion of binge eating’, Journal of Personality and Social Psychology, 55(4), pp. 588–598.
- Downs, J. (2023) ‘Untreatable or unable to treat? Eating disorders treatment’, The Lancet Psychiatry, 10(1), pp. 400-401.
- Eat Disorders Awareness Week (2026) Eating Disorders Awareness Week 2026. Available at: https://edaw.beateatingdisorders.org.uk/ (Accessed: 23 February 2026).
- Facebook (2024) Globally, eating disorders affect 2% to 5% of individuals during their lifetime. Available at: https://www.facebook.com/jamajournal/posts/globally-eating-disorders-affect-2-to-5-of-individuals-during-their-lifetime-and/1038970918277195 (Accessed: 23 February 2026).
- Fitzsimmons-Craft, E.E. (2011) ‘Social psychological theories of disordered eating in college women: Review and integration’, Clinical Psychology Review, 31(7), pp. 1224–1237.
- Government of Canada (2025) Eating disorders in teens: Information for parents and caregivers. Available at: https://www.canada.ca/en/public-health/services/publications/healthy-living/eating-disorders-teens-information-parents-caregivers.html (Accessed: 23 February 2026).
- Lemmens, T. (2025) ‘Canadian Medical Assistance in Dying: Provider Concentration, Policy Capture, and Need for Reform’, American Journal of Bioethics, 25(1), pp. 1-10.
- Lerman, K. (2025) ‘Safe spaces or toxic places? Content moderation and social dynamics of online eating disorder communities’, EPJ Data Science, 14(1), p. 575.
- Maung, H.H. (2023) ‘Externalist argument against medical assistance in dying for psychiatric illness’, Journal of Medical Ethics, 49(8), pp. 553-557.
- Mayo Clinic (2023) Eating disorders – Symptoms and causes. Available at: https://www.mayoclinic.org/diseases-conditions/eating-disorders/symptoms-causes/syc-20353603 (Accessed: 23 February 2026).
- Mullock, A. (2025) ‘Assisted dying, vulnerability, and the potential value of prospective legal authorization’, Medical Law Review, 33(2), pp. 1-20.
- National Council on Disability (2019) The Danger of Assisted Suicide Laws: Part of the Bioethics and Disability Series. Available at: https://www.ncd.gov/assets/uploads/docs/ncd-assisted-suicide-report-508.pdf (Accessed: 23 February 2026).
- National Eating Disorders Association (n.d.) Eating Disorder Statistics. Available at: https://www.nationaleatingdisorders.org/statistics (Accessed: 23 February 2026).
- National Institute for Health and Care Excellence (n.d.) Overview – Eating disorders. Available at: https://www.nhs.uk/mental-health/feelings-symptoms-behaviours/behaviours/eating-disorders/overview/ (Accessed: 23 February 2026).
- National Institute of Mental Health (n.d.) Eating Disorders: What You Need to Know. Available at: https://www.nimh.nih.gov/health/publications/eating-disorders (Accessed: 23 February 2026).
- Nawaz, F.A. (2024) ‘Social media use among adolescents with eating disorders: a double-edged sword’, Frontiers in Psychiatry, 15, p. 10884122.
- NHS (n.d.) Overview – Eating disorders. Available at: https://www.nhs.uk/mental-health/feelings-symptoms-behaviours/behaviours/eating-disorders/overview (Accessed: 23 February 2026).
- NHS Inform (2025) Avoidant restrictive food intake disorder (ARFID). Available at: https://www.nhsinform.scot/illnesses-and-conditions/mental-health/eating-disorders/avoidant-restrictive-food-intake-disorder-arfid (Accessed: 23 February 2026).
- NICE (2017) Eating disorders: recognition and treatment (NG69). Available at: https://www.nice.org.uk/guidance/ng69 (Accessed: 23 February 2026).
- NHS England (2026) Eating disorder services for children and young people: National guidance. Available at: https://www.england.nhs.uk/long-read/eating-disorder-services-for-children-and-young-people-national-guidance (Accessed: 23 February 2026).
- Nuffield Trust (2025) Assisted dying in practice. Available at: https://www.nuffieldtrust.org.uk/sites/default/files/2025-09/Nuffield%20Trust%20Assisted%20dying%20in%20practice_WEB-update.pdf (Accessed: 23 February 2026).
- Nuffield Trust (2025) Diverging paths: Assisted Dying in other countries. Available at: https://www.nuffieldtrust.org.uk/news-item/diverging-paths-how-other-countries-have-designed-and-implemented-assisted-dying (Accessed: 23 February 2026).
- Parliamentary Office of Science and Technology (2022) Assisted dying: Ethical debate and practical considerations. Available at: https://post.parliament.uk/research-briefings/post-pb-0047 (Accessed: 23 February 2026).
- Pehlivan, M.J. et al. (2022) ‘Models of care for eating disorders: findings from a rapid review’, Journal of Eating Disorders, 10(1), p. 671.
- Psychiatric Association (n.d.) What are Eating Disorders?. Available at: https://www.psychiatry.org/patients-families/eating-disorders/what-are-eating-disorders (Accessed: 23 February 2026).
- Right to Life UK (2025) Anorexia sufferers could access assisted suicide as MPs reject amendment. Available at: https://righttolife.org.uk/news/anorexia-sufferers-could-access-assisted-suicide-as-mps-reject-amendment (Accessed: 23 February 2026).
- Roff, C. (2024) Assisted death in eating disorders: a systematic review of cases and clinical rationales, Frontiers in Psychiatry, 15, p. 11322357.
- Royal College of Psychiatrists (n.d.) Avoidant/restrictive food intake disorder (ARFID). Available at: https://www.rcpsych.ac.uk/mental-health/mental-illnesses-and-mental-health-problems/avoidant-restrictive-food-intake-disorder-(arfid) (Accessed: 23 February 2026).
- Sanchez-Cerezo, J. et al. (2023) ‘What do we know about the epidemiology of avoidant/restrictive food intake disorder in children and adolescents? A systematic review of the literature’, European Eating Disorders Review, 31(2), pp. 226–246. doi: 10.1002/erv.2964.
- Scobie, S. (n.d.) Assisted dying in practice. Nuffield Trust.
- Scopetti, M. et al. (2023) ‘Assisted Suicide and Euthanasia in Mental Disorders’, Healthcare, 11(10), p. 1470.
- Sidani, J.E. et al. (2016) ‘The Association between Social Media Use and Eating Concerns among U.S. Young Adults’, Journal of the Academy of Nutrition and Dietetics, 116(9), pp. 1465–1472.
- UK Parliament (2025) Terminally Ill Adults (End of Life) Bill (28th January 2025). Available at: https://publications.parliament.uk/pa/cm5901/cmpublic/TerminallyIllAdults/memo/TIAB54.htm (Accessed: 23 February 2026).
- van Eeden, A.E. et al. (2021) ‘Incidence, prevalence and mortality of anorexia nervosa and bulimia nervosa’, Current Opinion in Psychiatry, 34(6), pp. 515–524. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC8500372/ (Accessed: 23 February 2026).
- Wang, T. et al. (2018) ‘Social interactions in online eating disorder communities: A network perspective’, PLoS ONE, 13(7), e0200800.